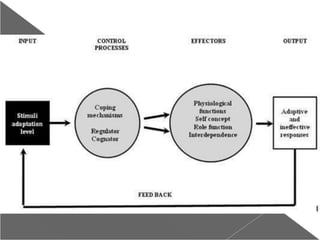
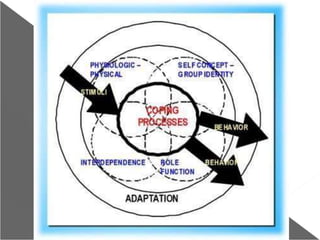
This document provides an overview of Sister Callista Roy's Adaptation Model of Nursing. It describes her background and career, the development and components of the model. The model views the person as an adaptive system who interacts with a changing environment. There are four modes of adaptation: physiological, self-concept, role function, and interdependence. Nursing aims to promote the person's adaptation through the use of the nursing process. The model has been influential in nursing education and has generated research to test its concepts.