This document provides information on various breathing exercises including their goals, techniques, indications, and precautions. Key points include:
- Breathing exercises aim to improve pulmonary function and endurance through techniques like diaphragmatic breathing and pursed lip breathing.
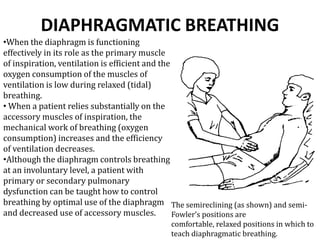
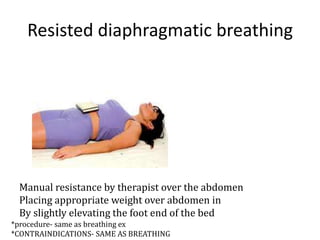
- Diaphragmatic breathing focuses on abdominal breathing to improve ventilation efficiency. Pursed lip breathing prolongs exhalation to slow breathing rate.
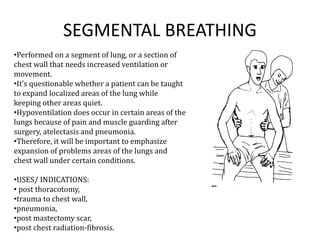
- Segmental breathing targets specific lung areas for those with issues post-surgery or illness.
- Indications for breathing exercises include COPD, cystic fibrosis, pneumonia, and other pulmonary disorders. Precautions aim to avoid hyperventilation or forced breathing.










![Physiotherapy in pulmonary_surgery[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonarysurgery1-230705093621-2b78f958-thumbnail.jpg?width=640&height=640&fit=bounds)
























































