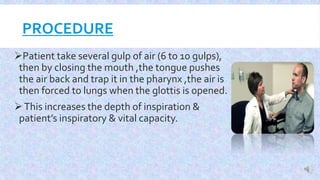
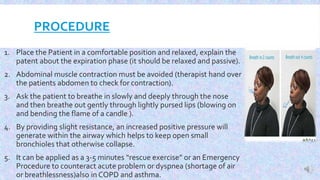
Breathing exercises, also called ventilatory training, are fundamental interventions for patients with pulmonary diseases. They can improve ventilation, increase cough effectiveness, prevent postoperative complications, and more. There are various types of breathing exercises, including diaphragmatic breathing, pursed lip breathing, and segmental breathing. Diaphragmatic breathing focuses on belly breathing to improve strength. Pursed lip breathing prolongs exhalation to slow breathing rate. Segmental breathing targets specific areas of the lungs that need more ventilation. Proper technique and positioning are important to teach patients how to correctly perform different breathing exercises.
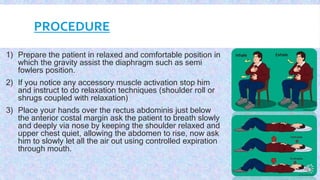






















![Neurophysiological facilitation of respiration [npf]](https://cdn.slidesharecdn.com/ss_thumbnails/neurophysiologicalfacilitationofrespirationnpf-180714163516-thumbnail.jpg?width=640&height=640&fit=bounds)















































