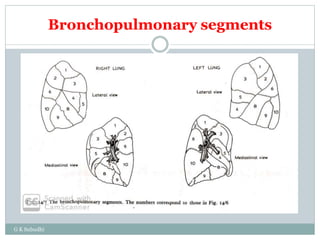
Postural drainage is a physiotherapy technique that utilizes gravity to assist in draining lung secretions by positioning the patient effectively for 15 to 20 minutes and engaging them actively. It incorporates manual techniques like percussion, shaking, and vibration to enhance airway clearance, particularly in patients with conditions such as cystic fibrosis, chronic bronchitis, or those recovering from surgery. Contraindications include conditions like active hemorrhage, unstable injuries, and respiratory issues that could worsen with the procedure.





























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








