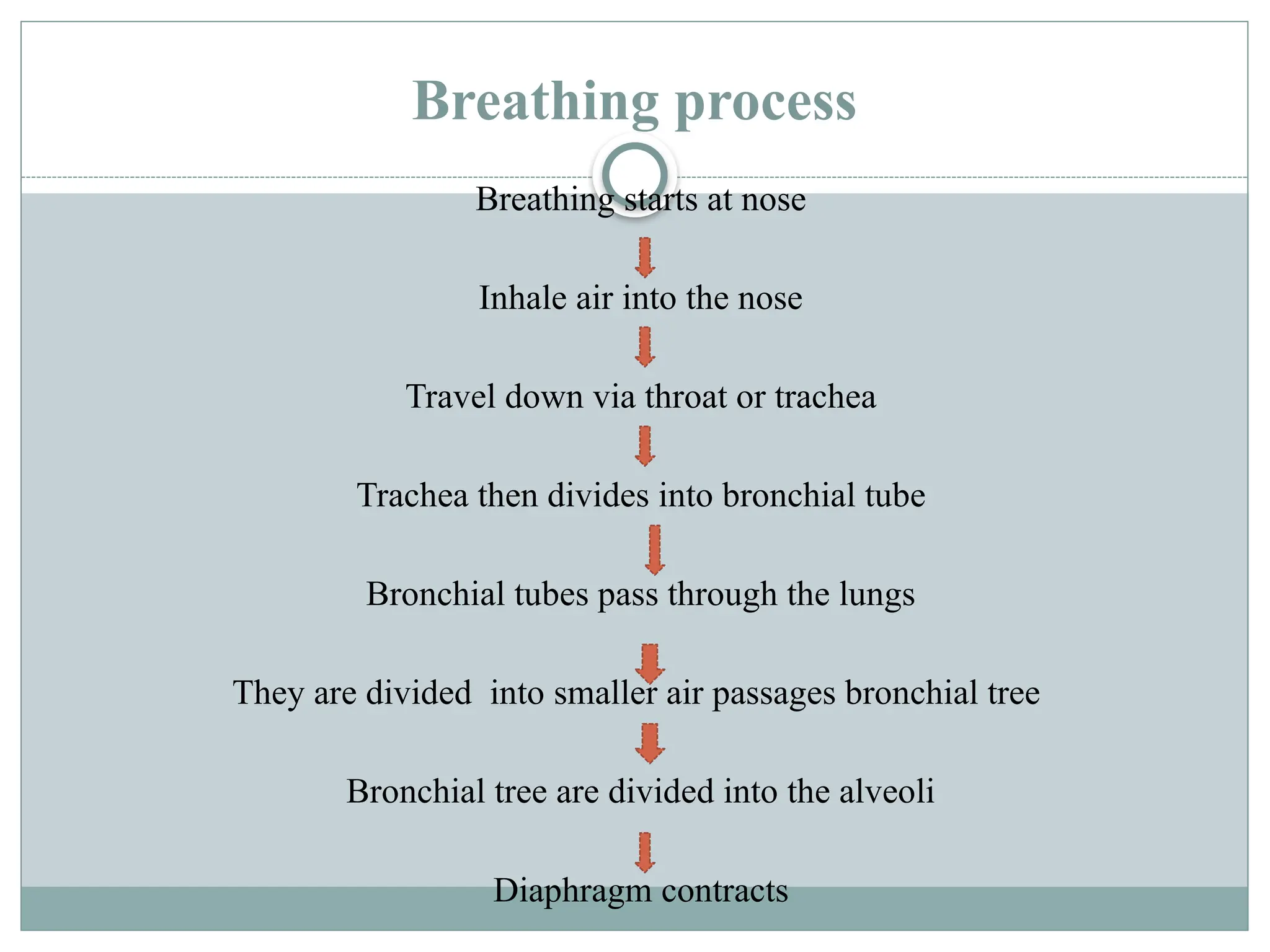
Breathing exercises are vital for managing pulmonary disorders and enhancing respiratory function. Techniques include diaphragmatic, glossopharyngeal, pursed-lip, and segmental breathing, each targeting specific muscle groups and improving areas like ventilation and oxygenation. Precautions should be taken to prevent forced expiration, hyperventilation, and inappropriately prolonged expirations.