Downloaded 425 times
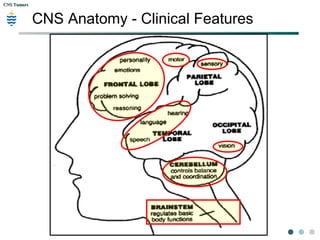
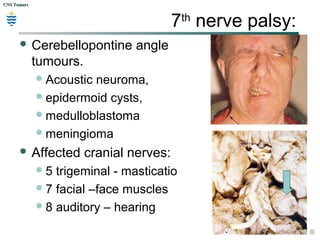
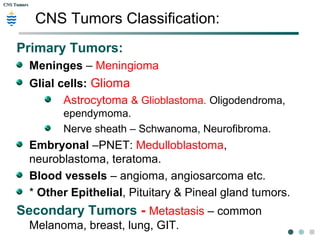
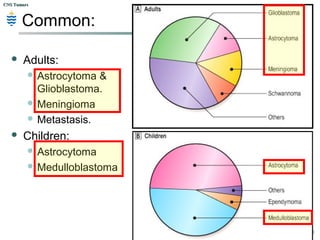
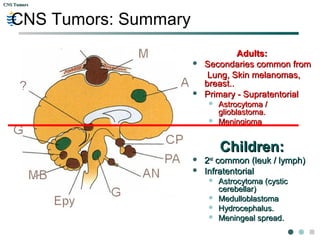
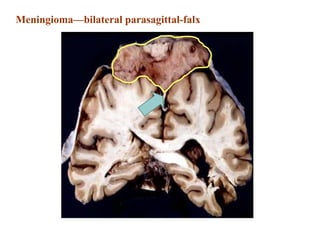
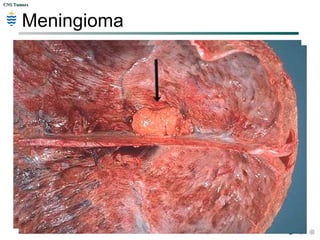
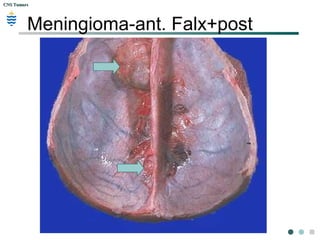
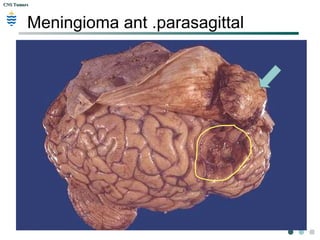
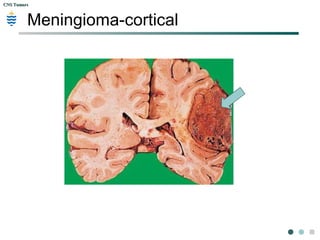
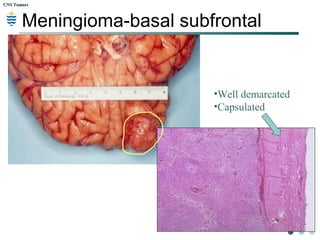
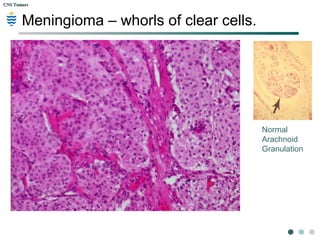
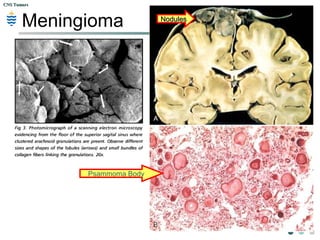
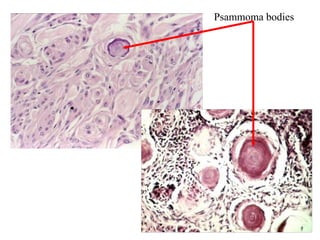
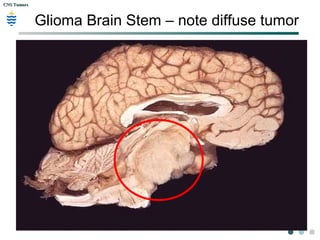
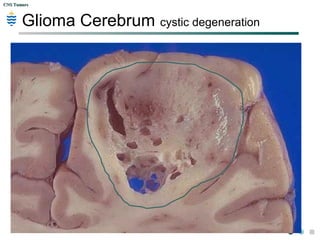
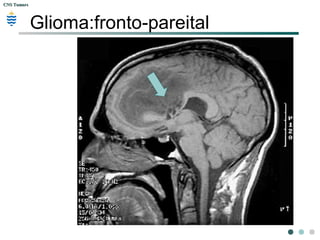
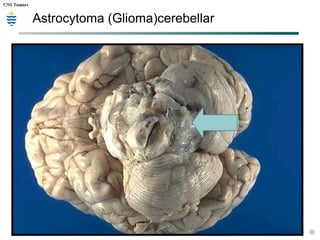
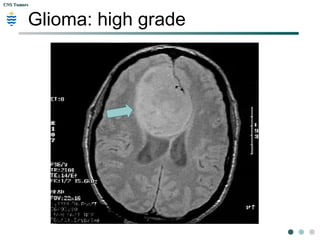
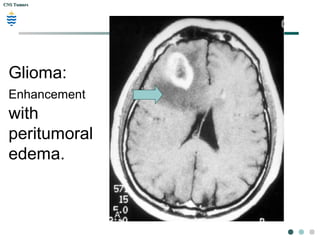
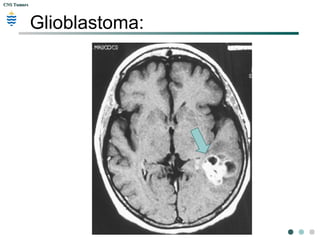
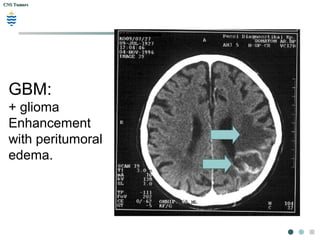
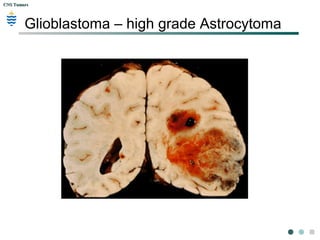
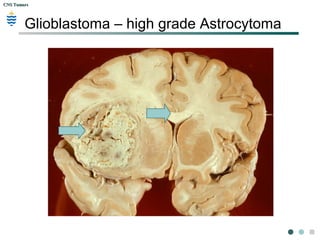
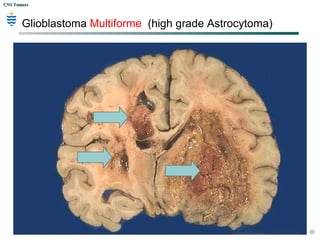
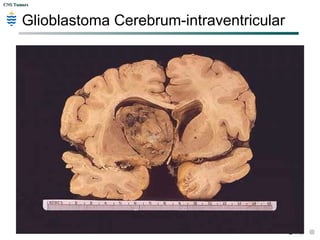
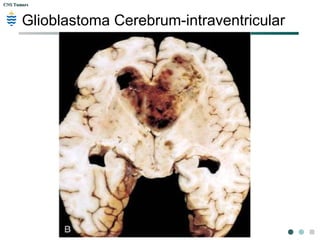
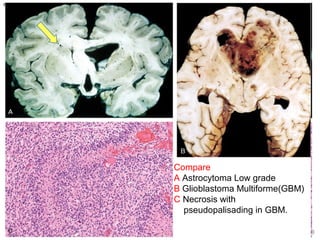
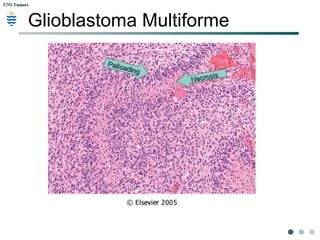
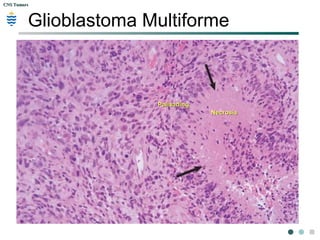
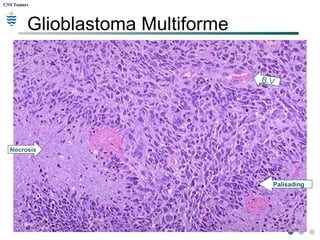
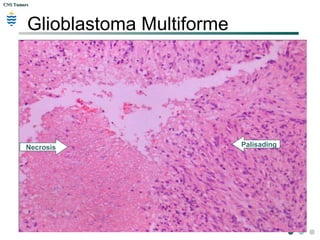
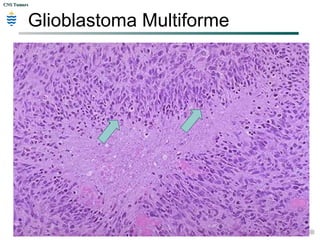
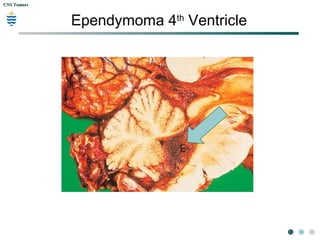
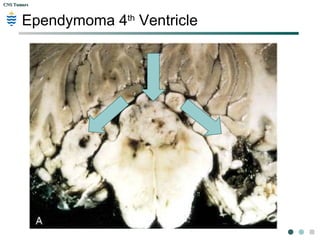
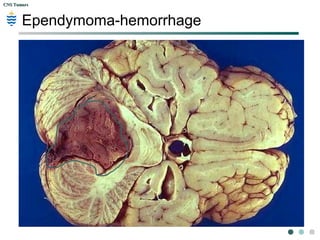
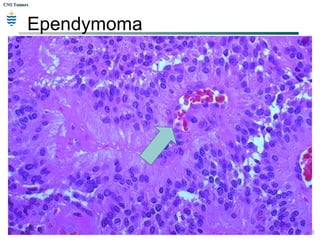
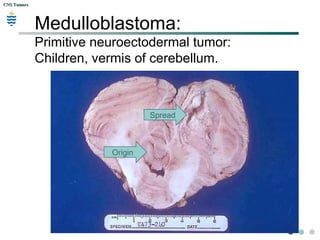
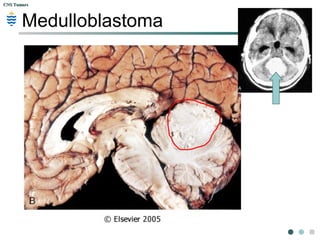
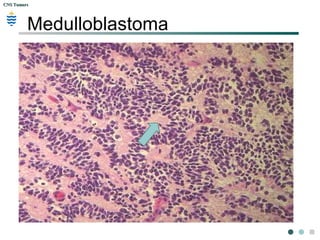
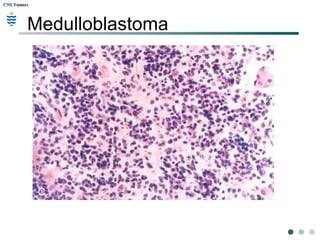
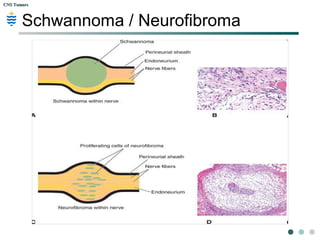
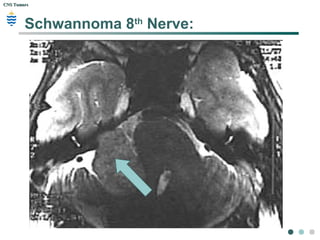
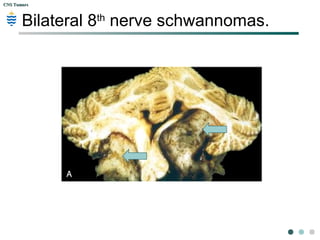
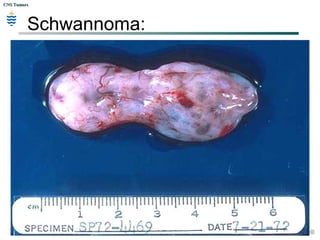
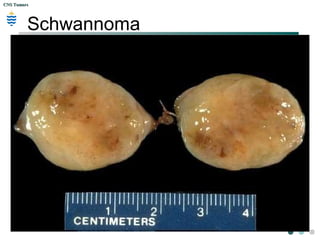
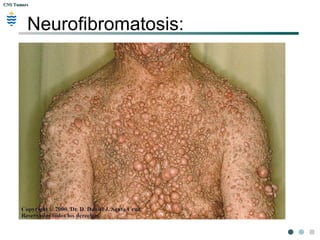
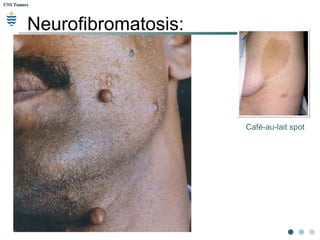
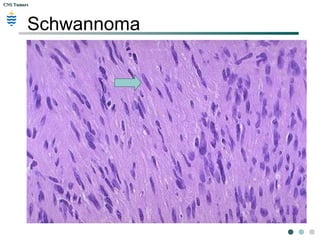
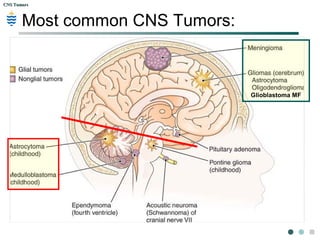
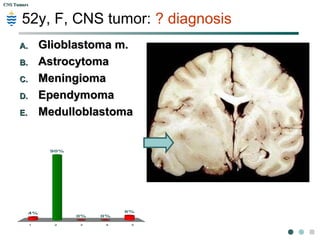
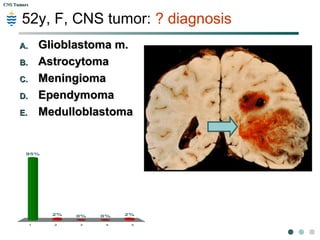
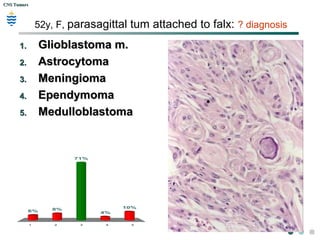
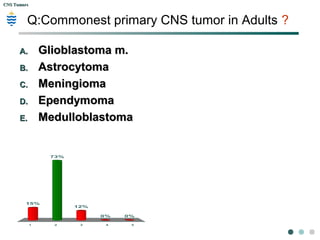
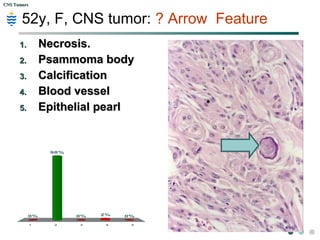
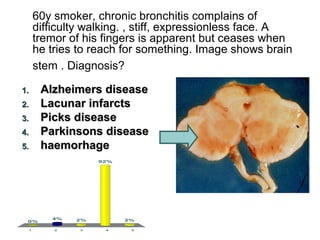
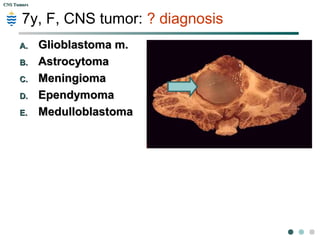
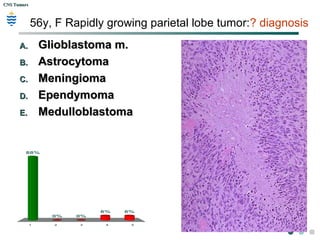
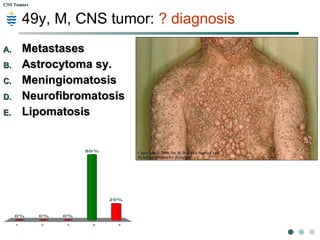
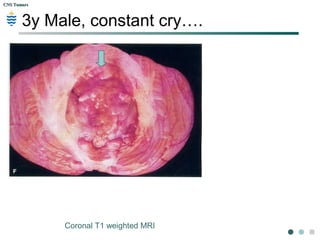

The document discusses central nervous system (CNS) tumors. It provides information on different types of primary and secondary brain tumors seen in adults and children, including meningiomas, gliomas such as astrocytomas and glioblastomas, medulloblastomas, and nerve sheath tumors. Key points covered include the typical locations, presentations, pathological features, and distinguishing characteristics of common CNS tumors.

























































































