Downloaded 274 times


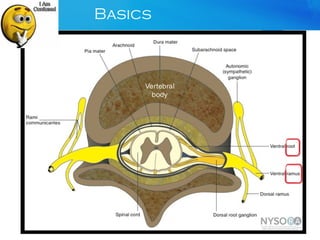
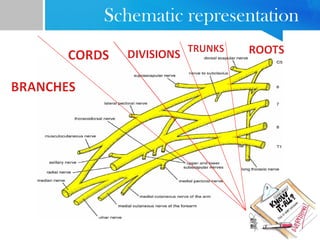
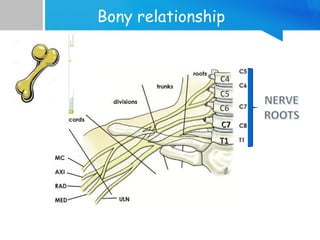
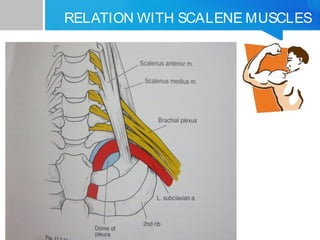
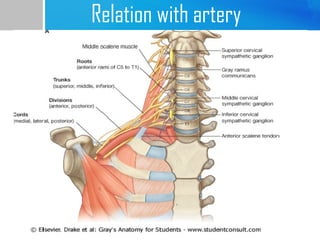
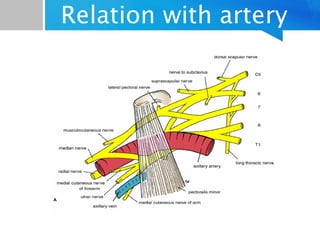
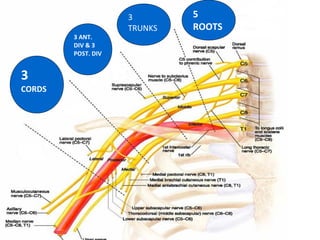
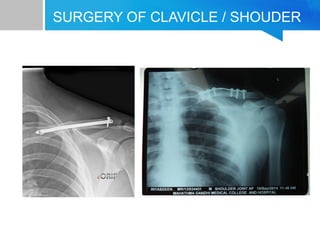
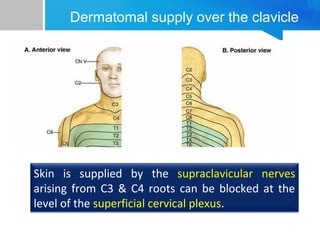
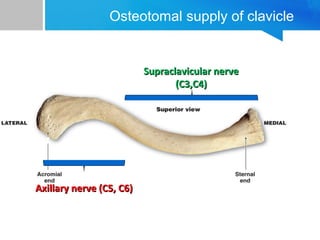
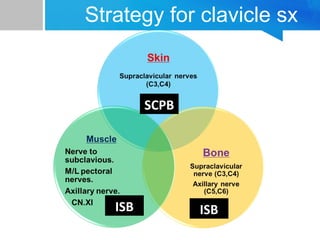

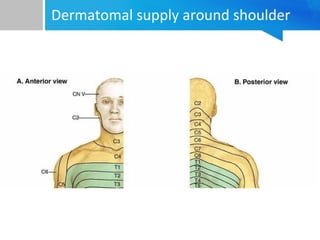
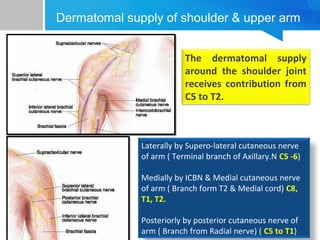
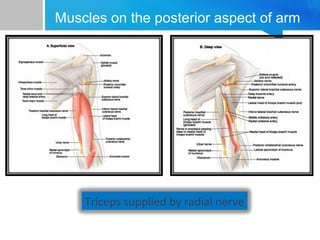
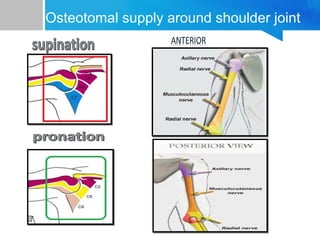
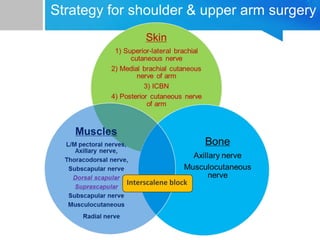
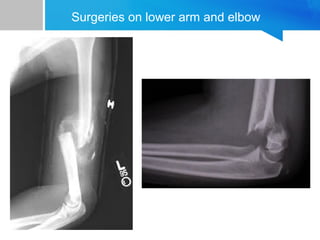

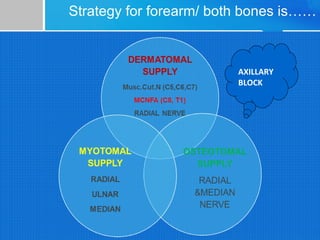

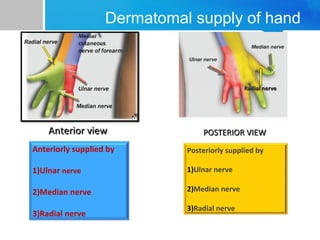
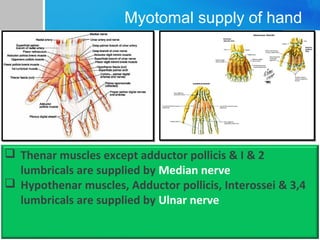
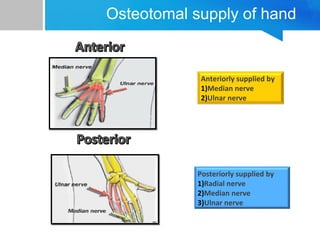

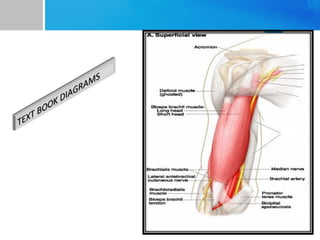
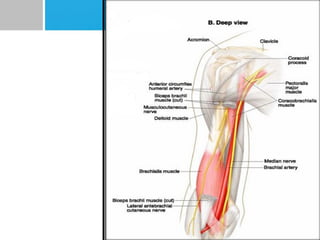
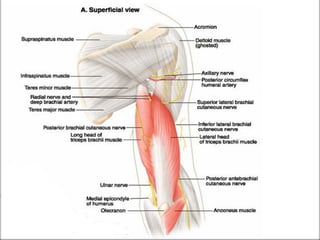
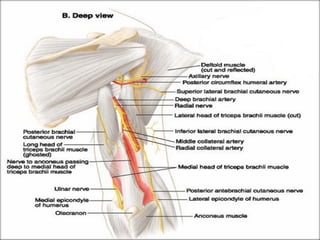

This document provides an overview of regional strategies for upper limb surgeries. It begins with an introduction to brachial plexus anatomy and dermatomal, muscular and osteotomal supply to the clavicle, shoulder, upper arm, elbow, forearm and hand. For each region, relevant surgical approaches and recommended regional anesthesia techniques are described, such as interscalene block for shoulder/upper arm surgeries and axillary block for forearm procedures. The document aims to guide anesthesia providers in selecting the appropriate nerve block based on the specific limb location being operated.





































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















