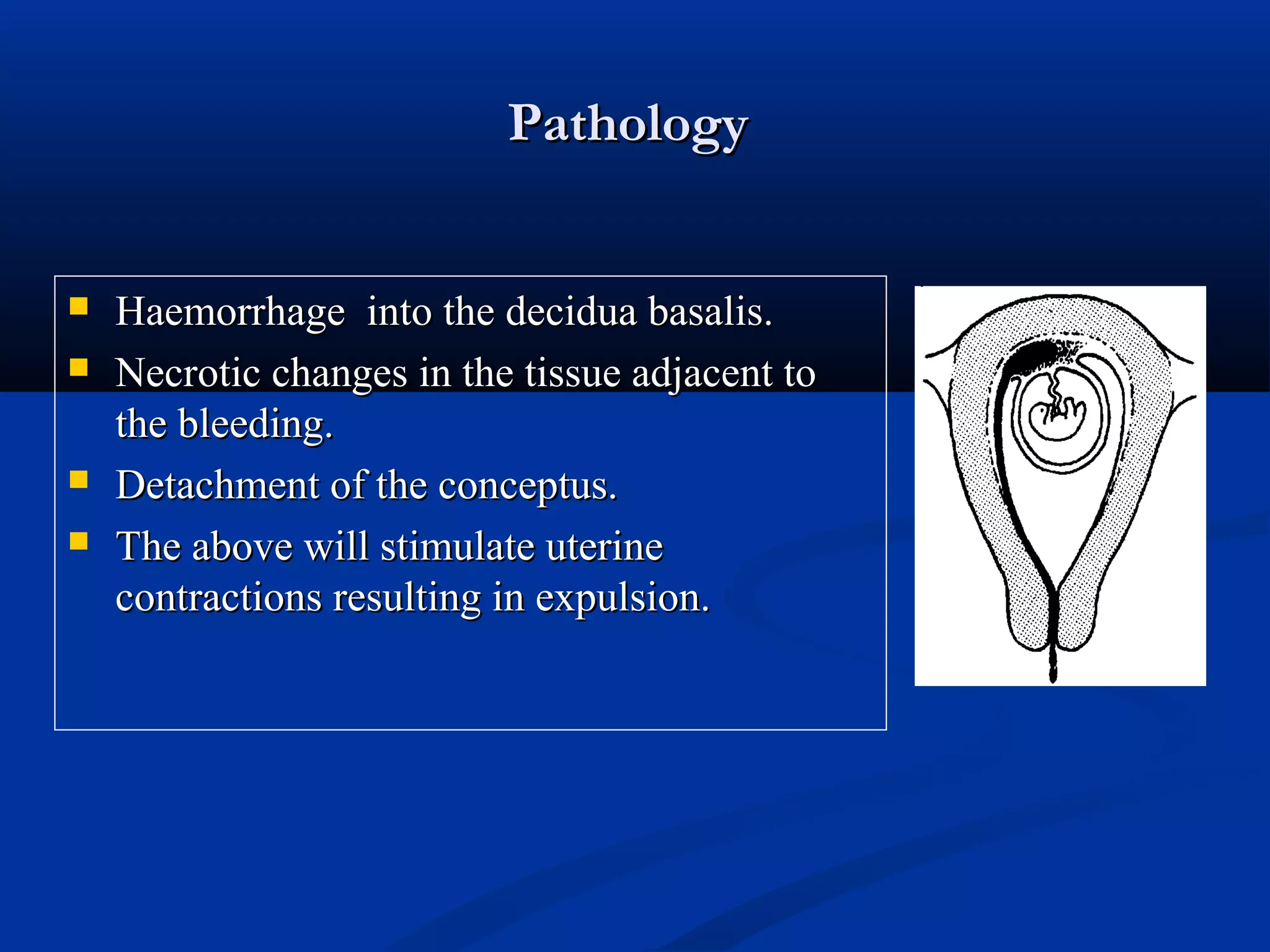
Early bleeding in pregnancy can be caused by ectopic pregnancy, abortion, or hydatidiform mole. Abortion, also called miscarriage, is the spontaneous loss of a fetus before 24 weeks gestation and can be caused by fetal chromosome abnormalities in 50% of cases, uterine abnormalities like fibroids, endocrine issues like diabetes, infections, or environmental factors. The types of abortion include threatened, inevitable, incomplete, complete, and missed. Missed abortion features the gradual disappearance of pregnancy signs and symptoms despite an empty uterus seen on ultrasound. Management depends on the type but may include medication, dilation and evacuation, or expectant management.