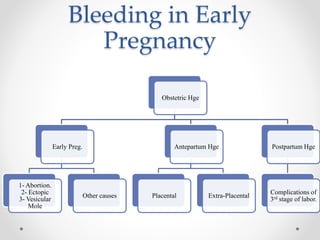
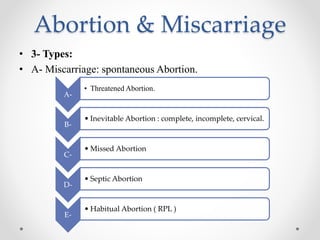
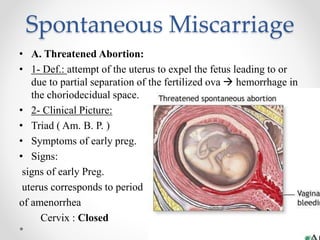
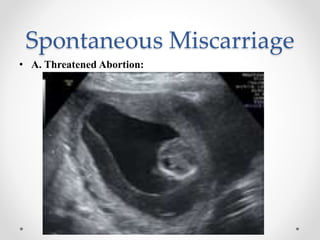
This document discusses bleeding in early pregnancy and covers various topics including causes of obstetric hemorrhage, definitions and types of miscarriage, risk factors for miscarriage, ectopic pregnancy, and recurrent pregnancy loss. Specifically, it defines threatened, inevitable, complete, incomplete, cervical, and missed miscarriages as well as septic abortion. For each type of miscarriage, the document outlines clinical presentation, investigations, complications and treatment approaches. It also briefly discusses the definition, incidence, etiology, clinical picture and treatment of recurrent pregnancy loss.

























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














