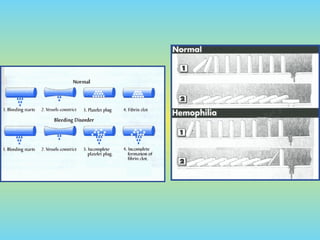
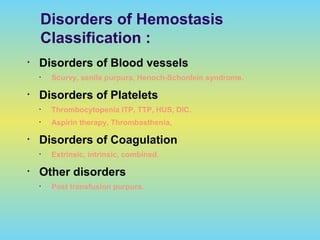
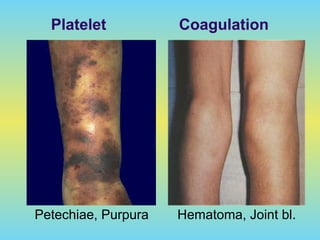
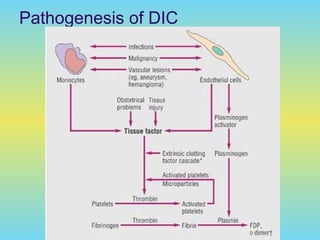
1) Bleeding disorders can involve vascular, platelet, or coagulation disorders and cause symptoms like bruising, bleeding, and prolonged bleeding from minor cuts.
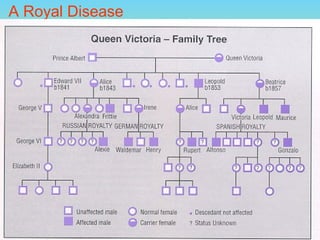
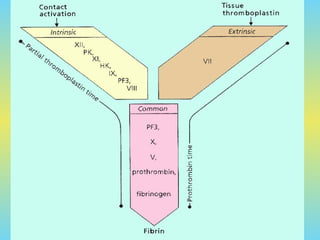
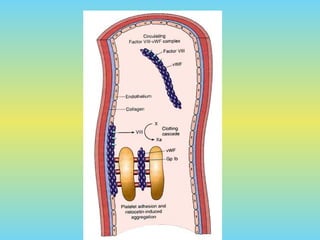
2) Important bleeding disorders discussed include hemophilia A (factor VIII deficiency), hemophilia B (factor IX deficiency), von Willebrand disease (a disorder of the von Willebrand clotting factor), and fibrinogen deficiency.
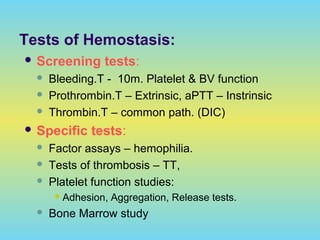
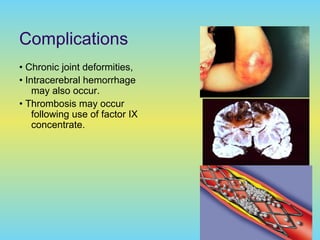
3) These disorders are diagnosed through tests of bleeding time and clotting factor levels and activity. Treatment involves replacing the missing clotting factor through products like cryoprecipitate, desmopressin, or clotting factor concentrates.








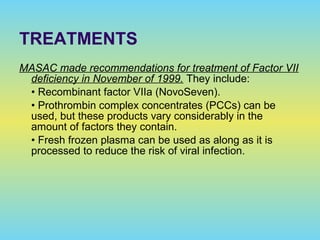
![Chronic DIC
Without thromboembolism
No specific therapy needed but prophylactic drugs
(eg, low-dose heparin, low-molecular-weight heparin)
With thromboembolism
Heparin or low-molecular-weight heparin, trial of warfarin
sodium (Coumadin).
*Some patients respond to warfarin, others do not. Use of
low-molecular-weight heparin for prolonged periods has
potential hazards and is expensive but can be useful when
warfarin therapy fails despite good control (international
normalized ratio [INR], 2-3).](https://image.slidesharecdn.com/090-190209054915/85/Bleeding-Disorders-Causes-Types-and-Diagnosis-96-320.jpg)

















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





