Downloaded 10 times











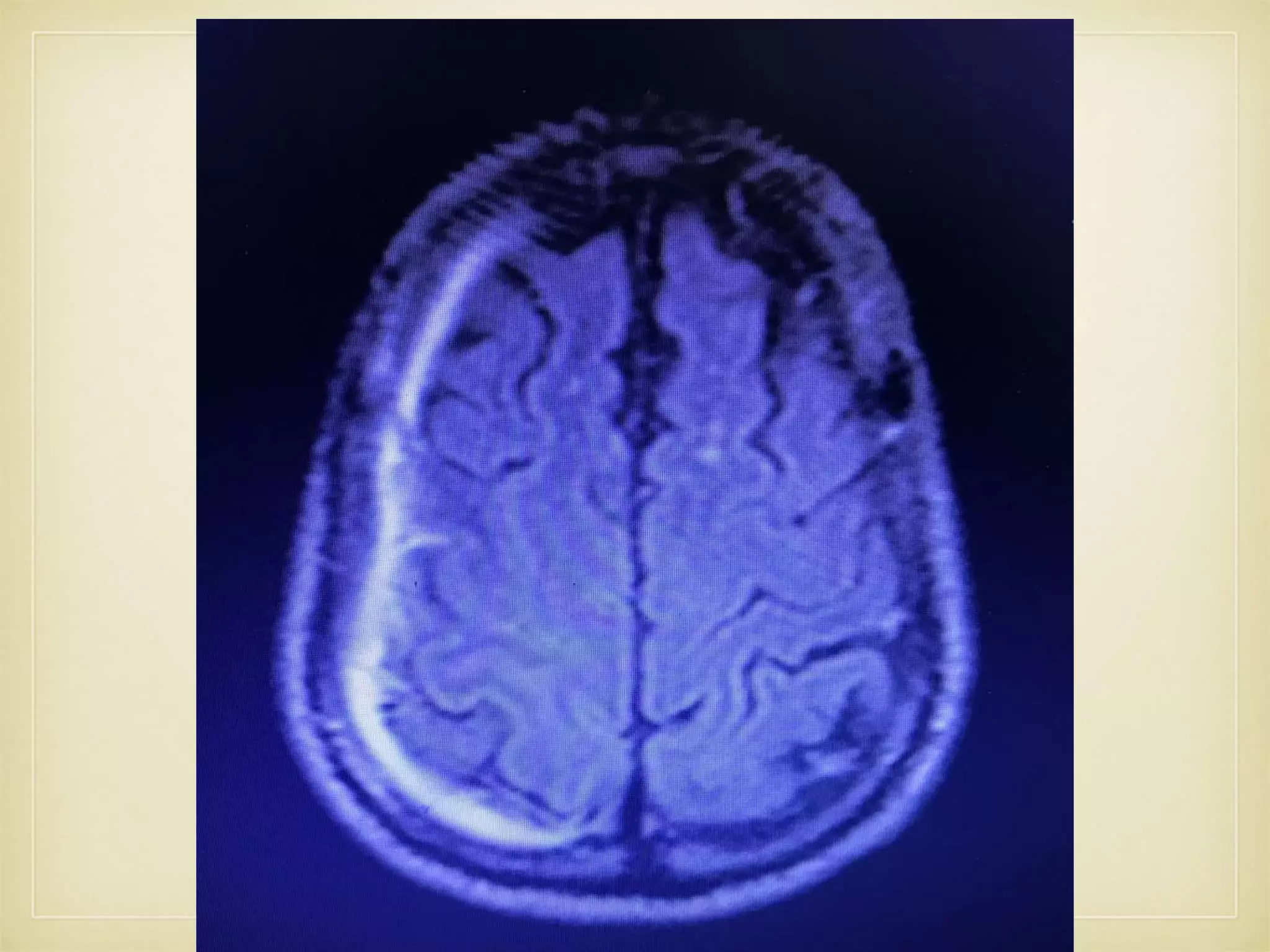

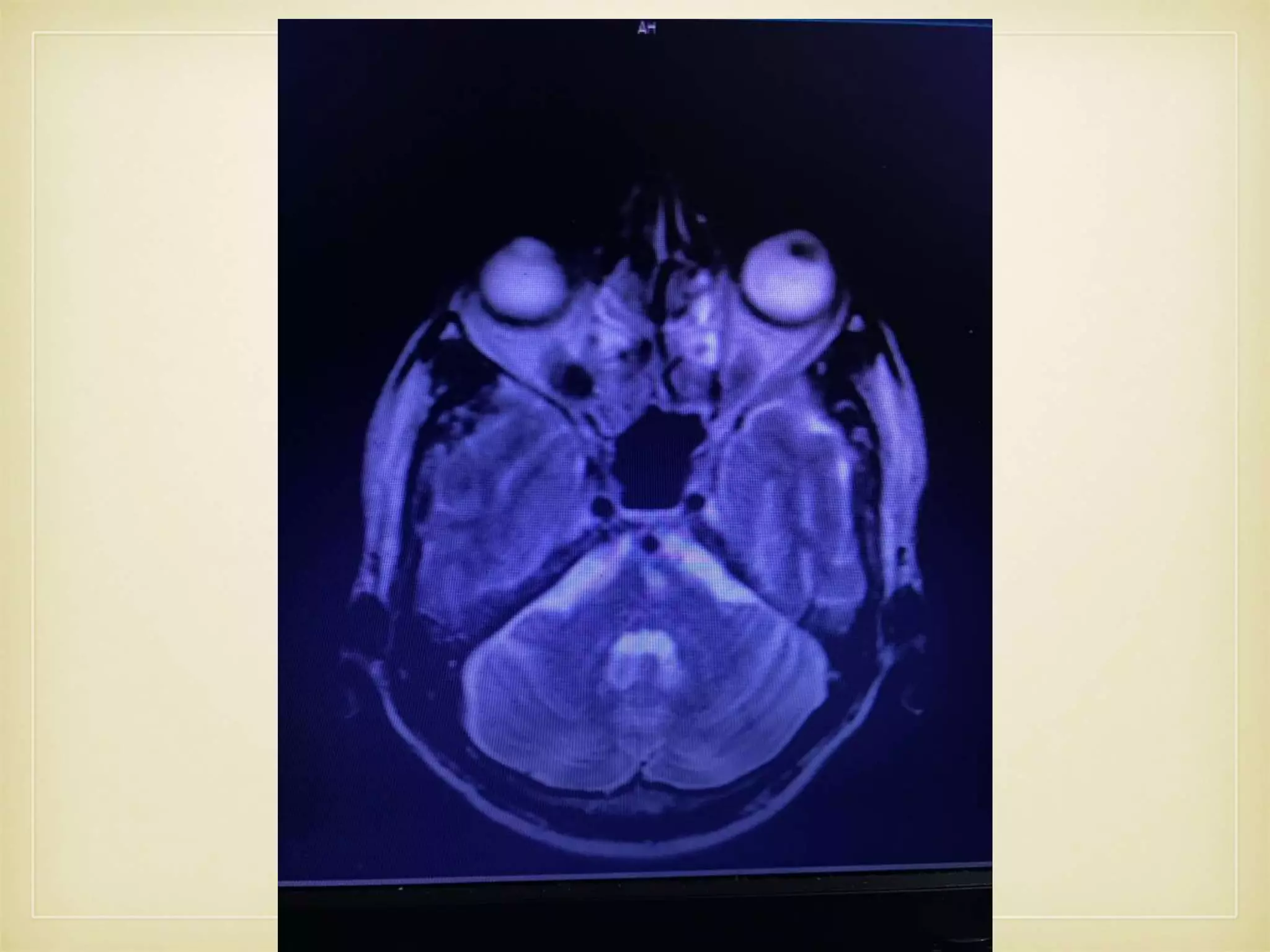





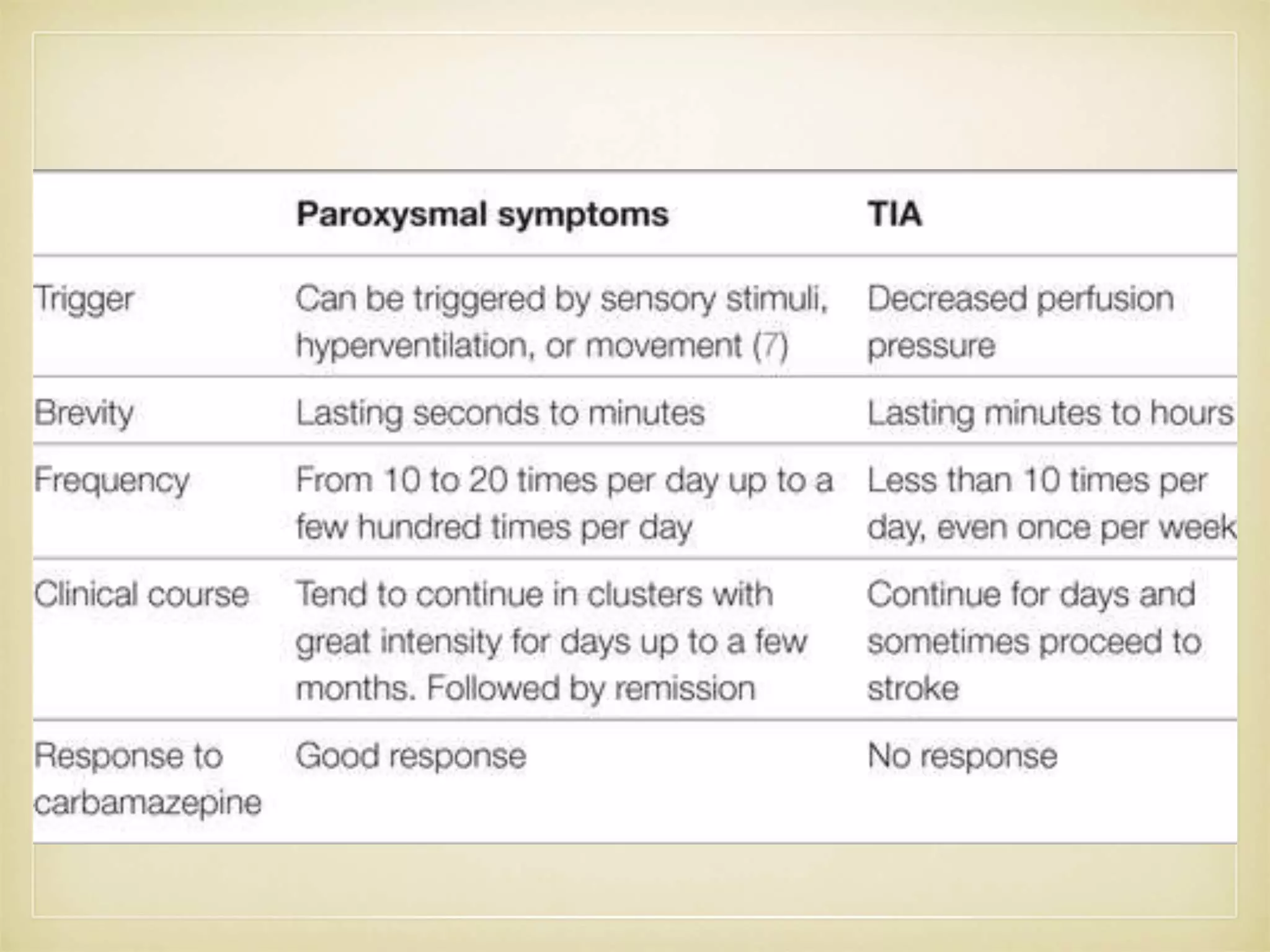





This document presents the case of a 68-year-old male who presented with fever and loss of consciousness followed by a fall and weakness on his right side. He experienced brief episodes of dysarthria lasting 5-10 minutes associated with swallowing difficulty. Imaging showed a subdural hematoma in the right frontal-temporal-parietal region. He was treated and improved but later experienced paroxysmal dysarthria again, which was controlled with anti-seizure medication. The causes and potential mechanisms of his paroxysmal dysarthria are discussed.





















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)

