Download to read offline

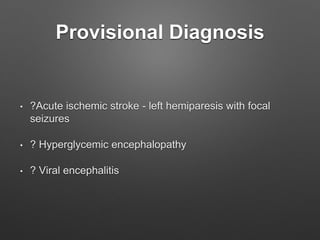
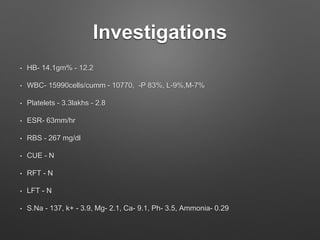

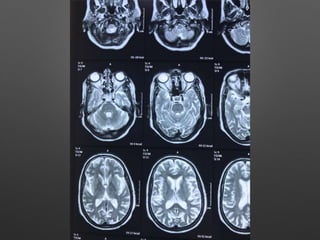
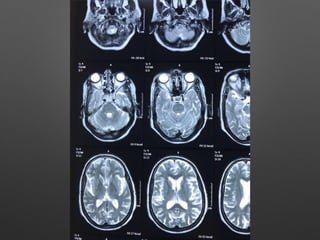
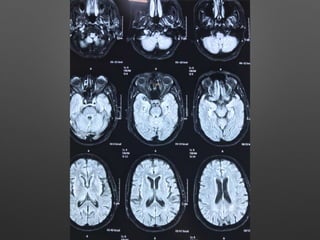
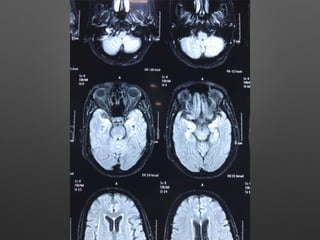
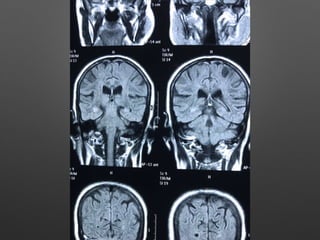

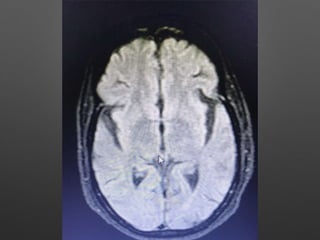
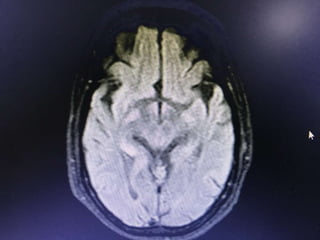
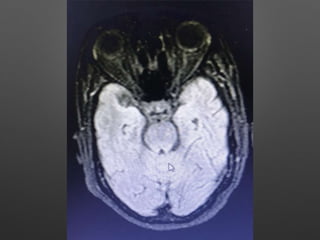
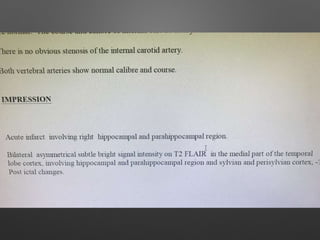

A 71-year-old diabetic woman presented to the emergency room with sudden onset of irrelevant speech and behavior. She experienced two episodes of focal seizures involving her left side. On examination, she was disoriented with mild left-sided weakness. Tests showed elevated blood sugar and signs of inflammation. The doctors' provisional diagnoses included acute ischemic stroke, viral encephalitis, or hyperglycemic encephalopathy. She was treated with anti-seizure medications and oral hypoglycemic agents, which improved her sensorium and strength.























































































