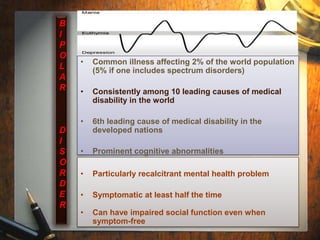
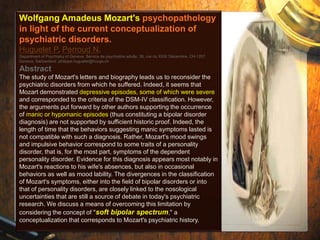
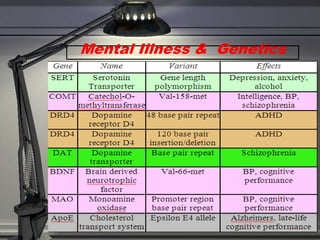
This document discusses the history, diagnosis, and challenges of bipolar disorder. It traces the recognition and understanding of the disorder back to ancient Greek physicians like Hippocrates and Aretaeus. In the late 19th century, Emil Kraepelin defined manic-depressive illness and distinguished it from schizophrenia. The concept of bipolar disorder was further developed in the 20th century. It remains a highly prevalent mental illness worldwide, with genetic and biochemical contributors as well as structural brain abnormalities implicated in its pathophysiology. Managing bipolar disorder long-term poses ongoing challenges.
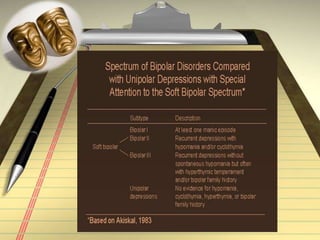
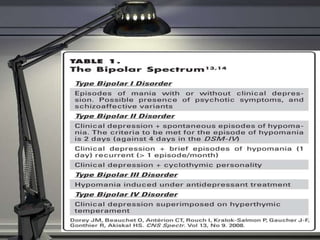
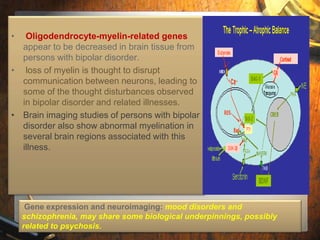
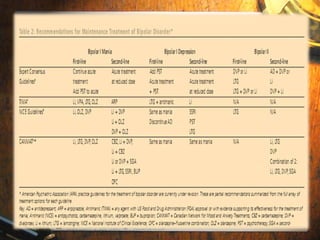
![Akiskal's Schema of Bipolar Subtypes
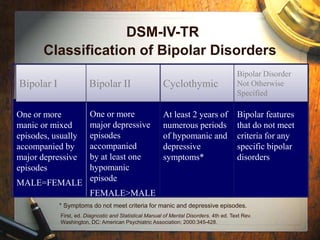
(Psychiatric Clinics of North America 22:3, September 1999; Medscape Family
Medicine, 2005;7[1])
Bipolar I: full-blown mania
Bipolar I ½: depression with protracted hypomania
Bipolar II: depression with hypomanic episodes
Bipolar II ½: cyclothymic disorder
Bipolar III: hypomania due to antidepressant drugs
Bipolar III ½: hypomania and/or depression associated with
substance use
Bipolar IV: depression associated with hyperthymic temperament
Bipolar V: recurrent depressions that are admixed with dysphoric
hypomania
Bipolar VI: late onset depression with mixed mood features,
progressing to a dementia-like syndrome](https://image.slidesharecdn.com/bipolardisorder20112-141215005427-conversion-gate02/85/Bipolar-disorder-16-320.jpg)







































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


