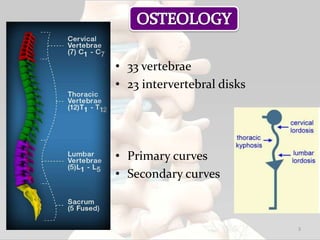
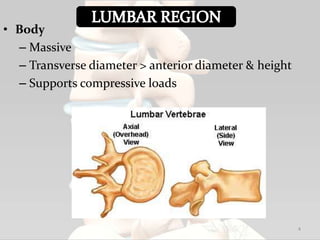
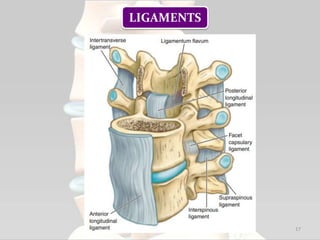
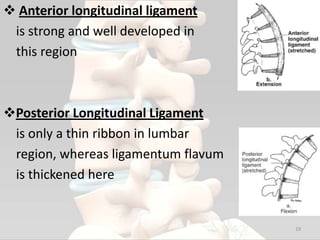
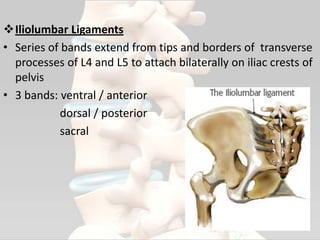
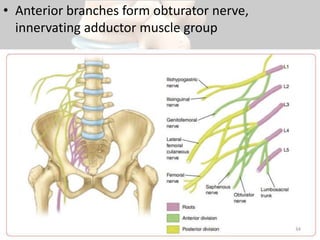
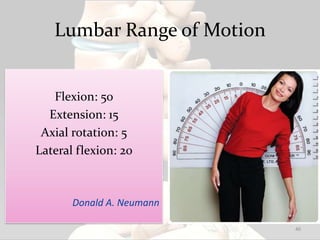
1. The document discusses the anatomy and biomechanics of the lumbar spine, including osteology, articulations, ligaments, muscles, nerves and typical ranges of motion.
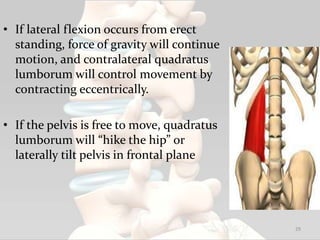
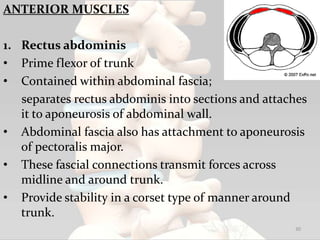
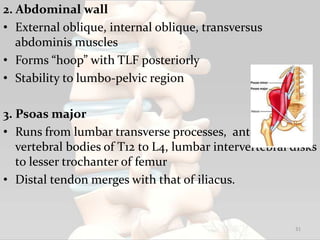
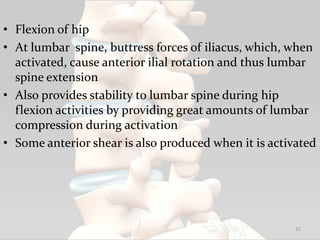
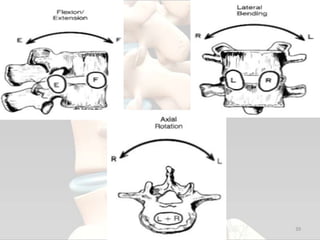
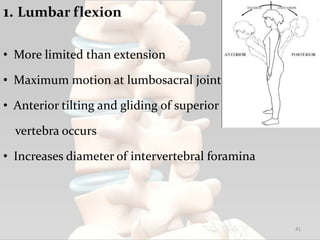
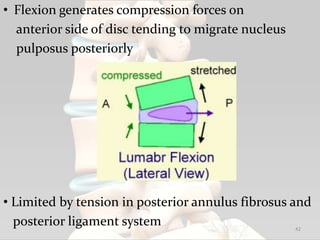
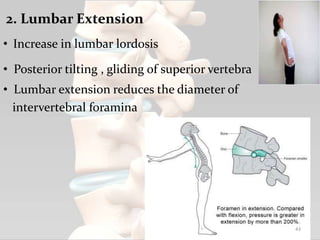
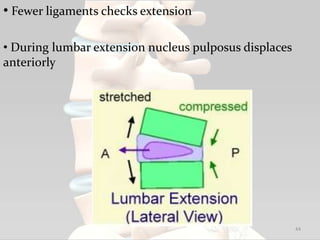
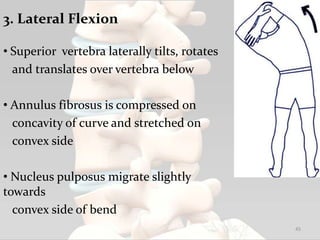
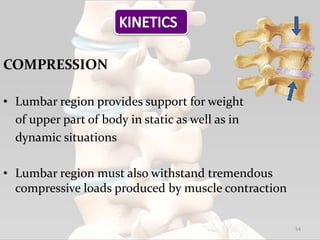
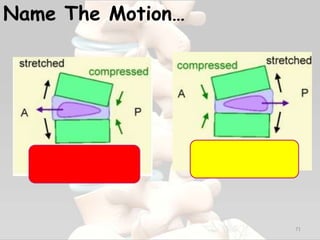
2. Key biomechanical concepts covered are the compression, shear, and coupling forces experienced during flexion, extension, lateral flexion and rotation.
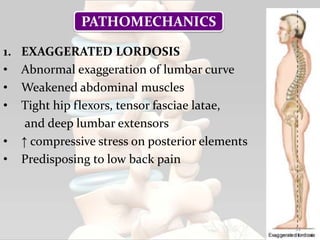
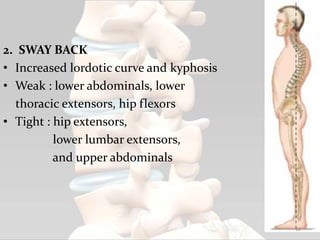
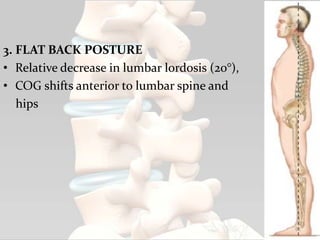
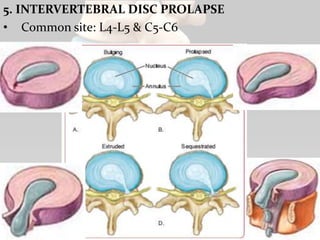
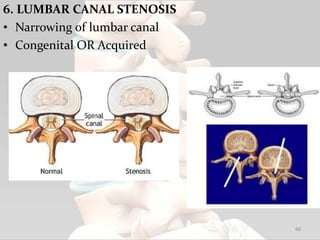
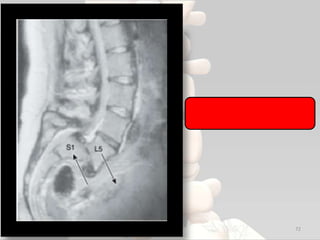
3. Common pathomechanics like exaggerated lordosis, sway back posture, and intervertebral disc prolapse are explained.