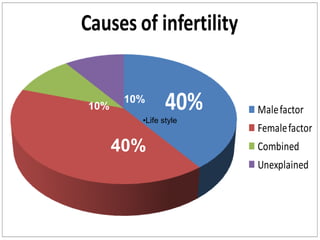
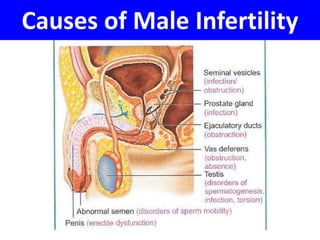
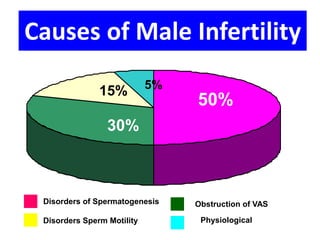
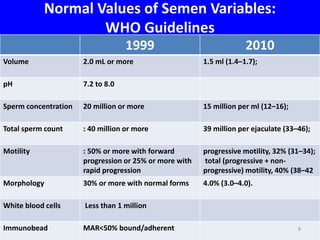
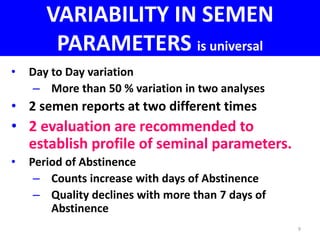
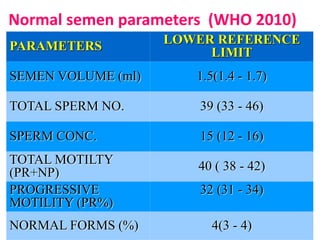
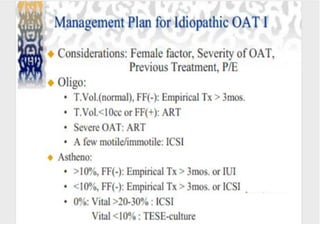
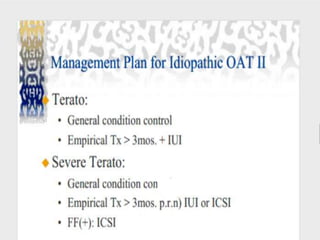
This document summarizes a panel discussion on male infertility and the management of oligo astheno teratospermia (OAT). The panel included urologists, IVF experts, and gynaecologists who discussed topics such as the causes of male infertility, recent WHO criteria for semen analysis, what constitutes OAT, specific and idiopathic causes of OAT, how smoking affects fertility, and the steps in evaluating a male for infertility including history, examination, semen analysis, hormone assays, ultrasound, and additional tests or procedures when indicated.