Downloaded 49 times
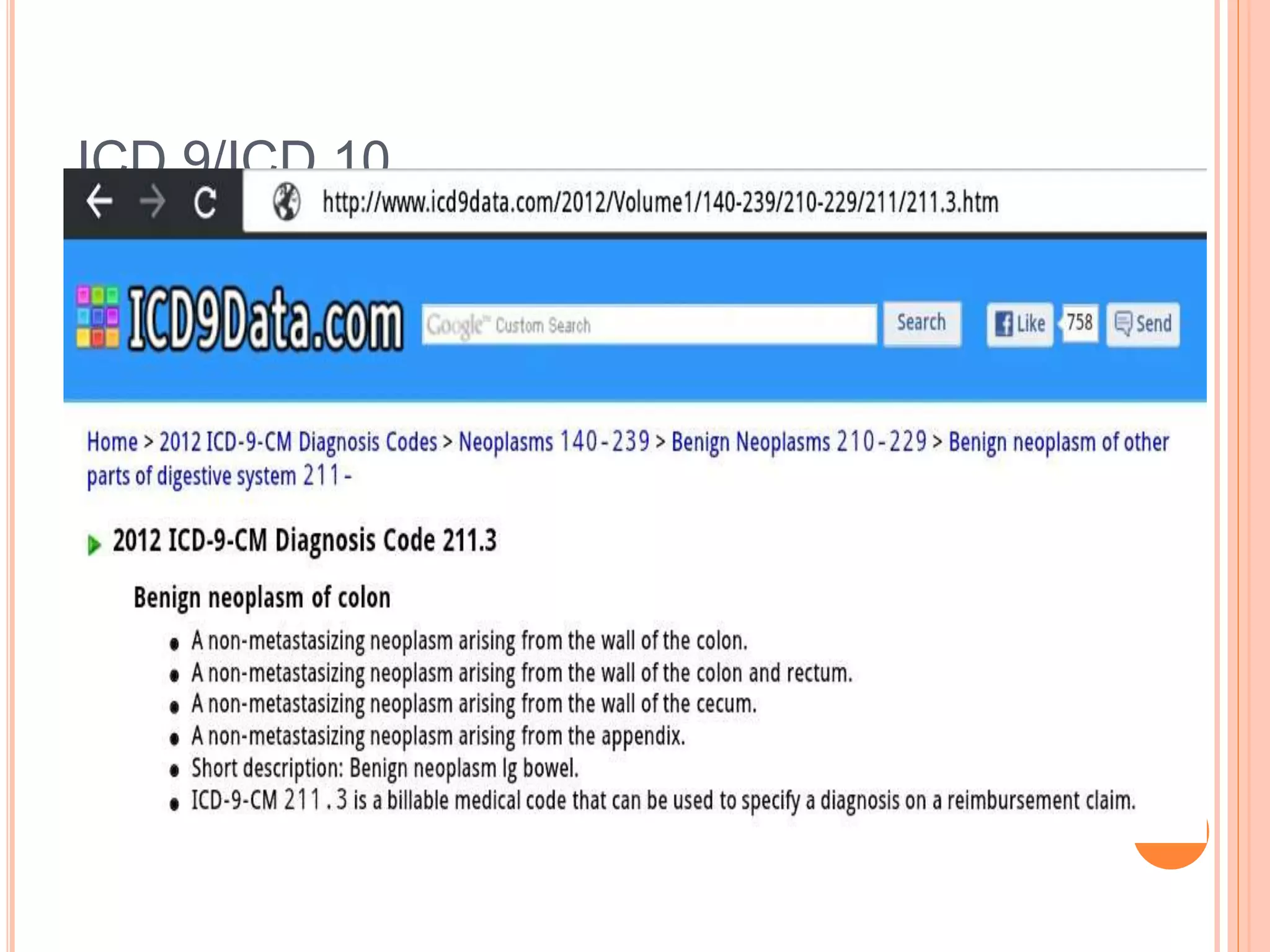
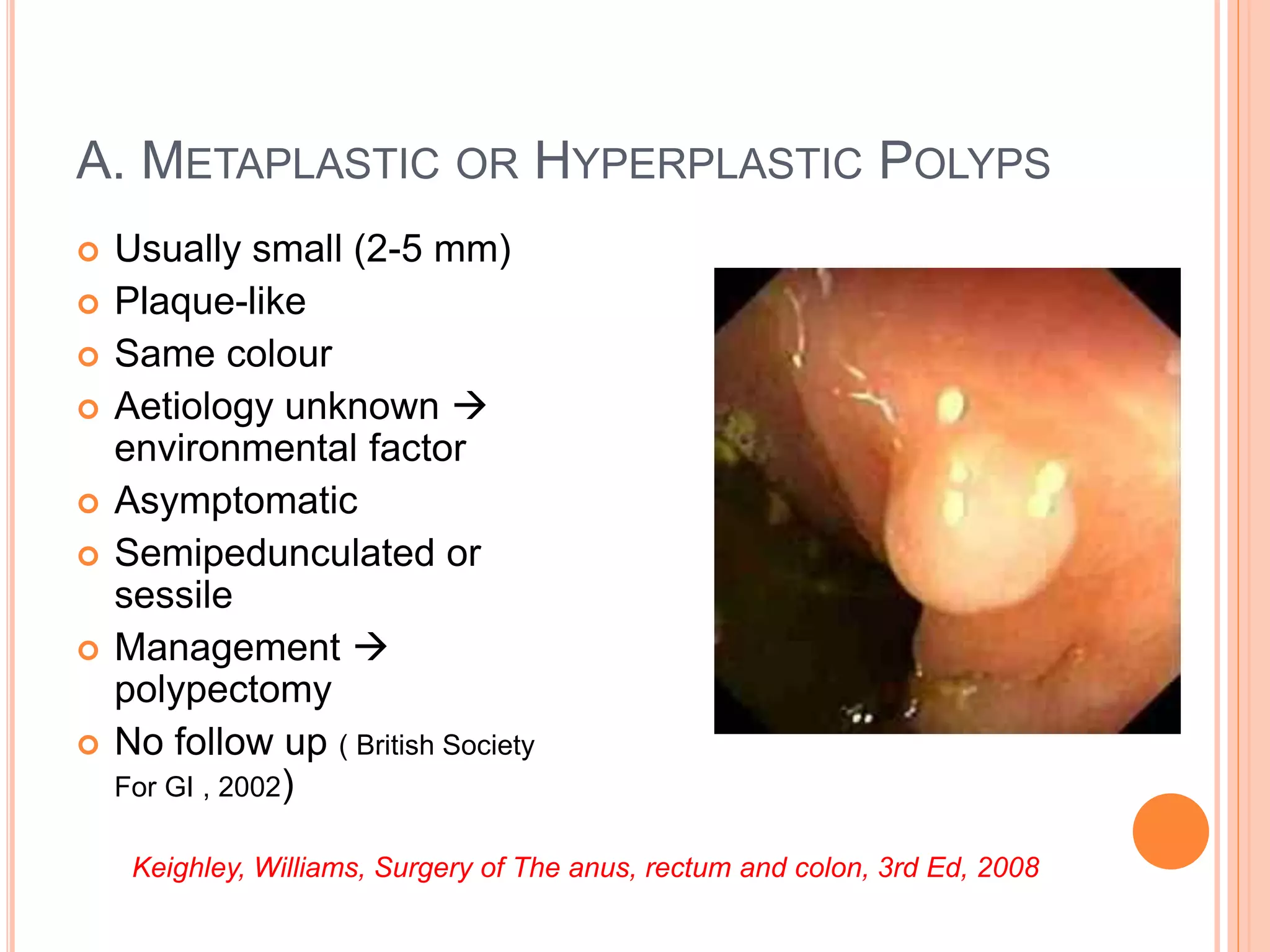









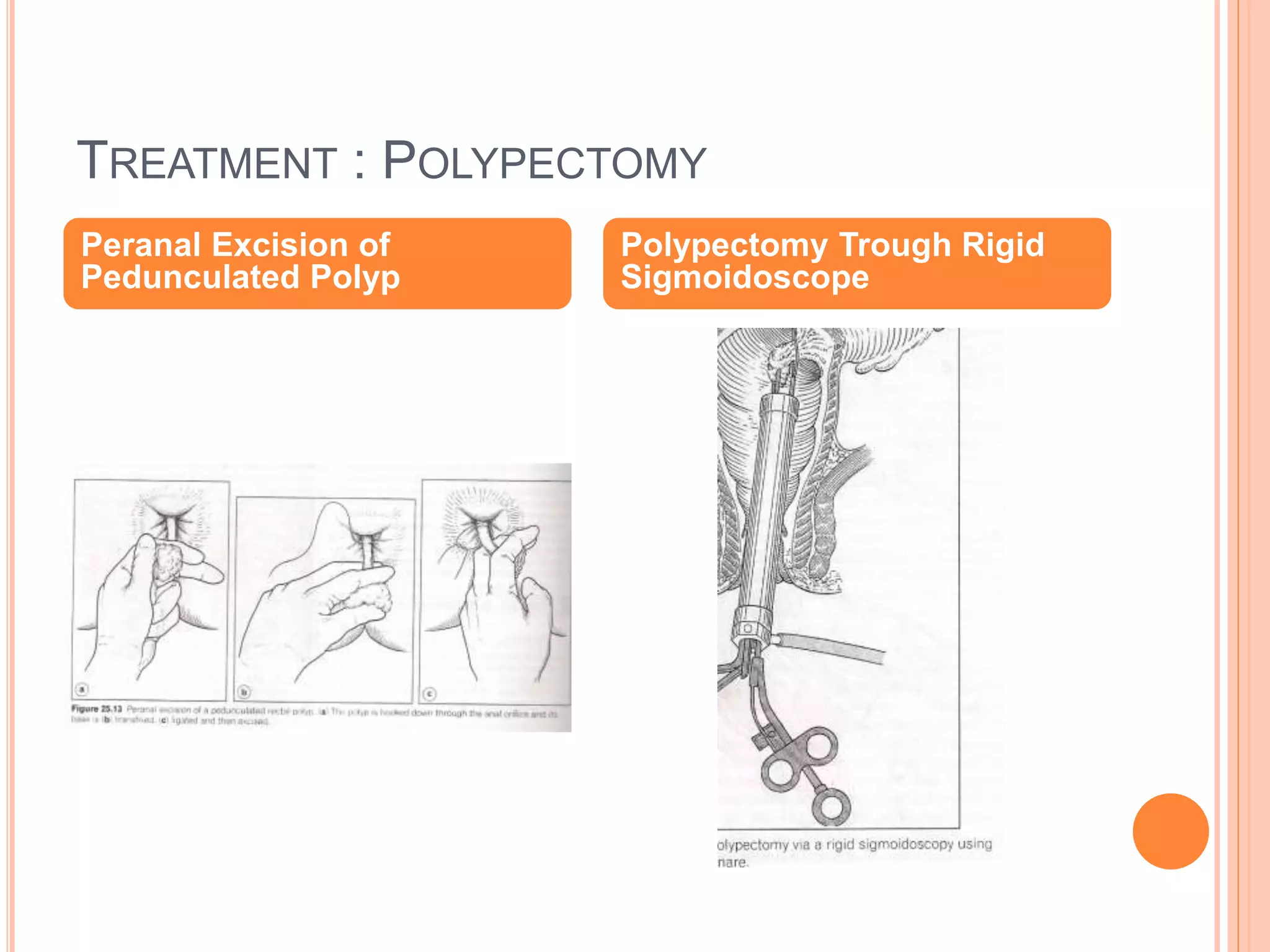
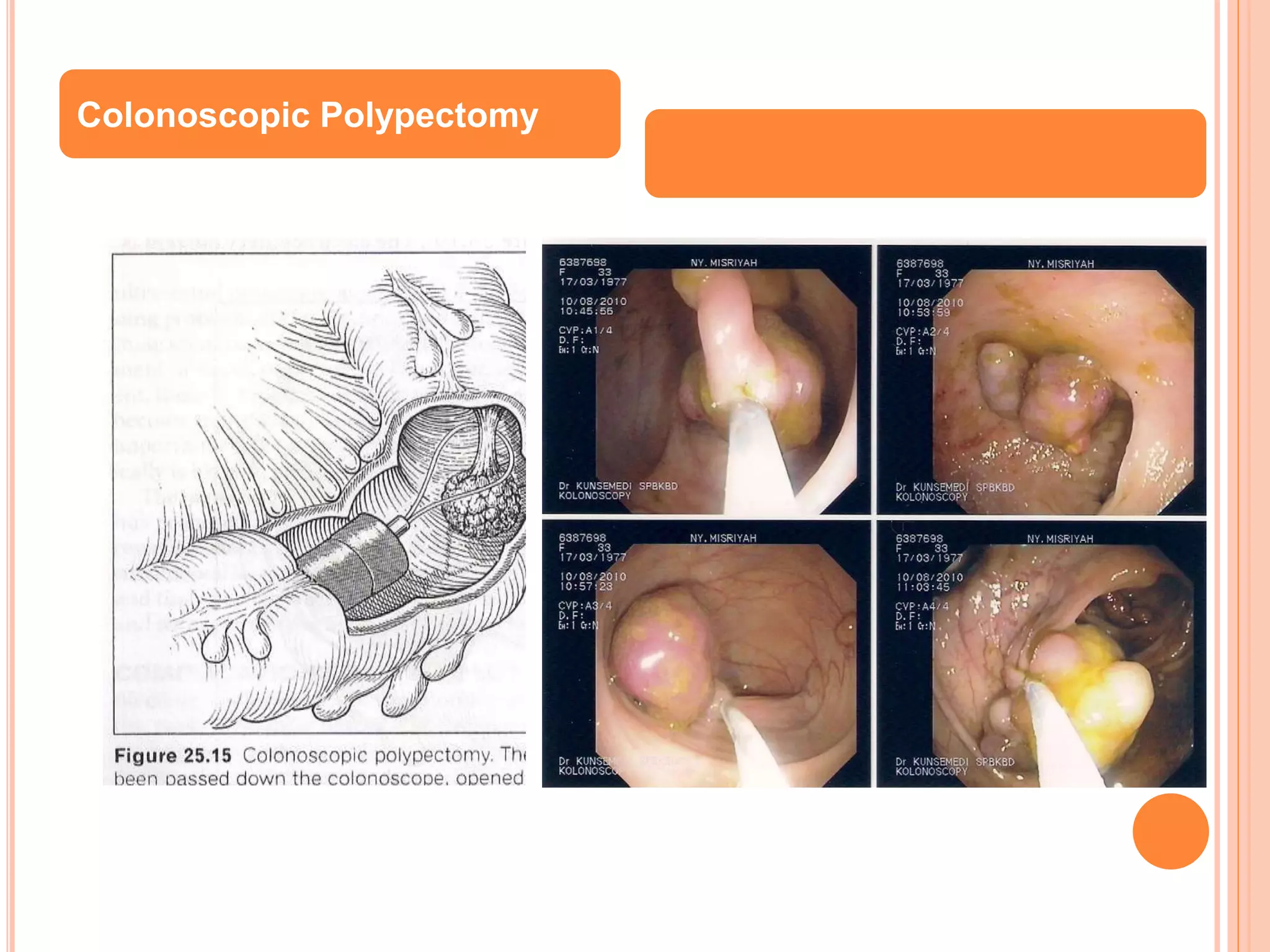


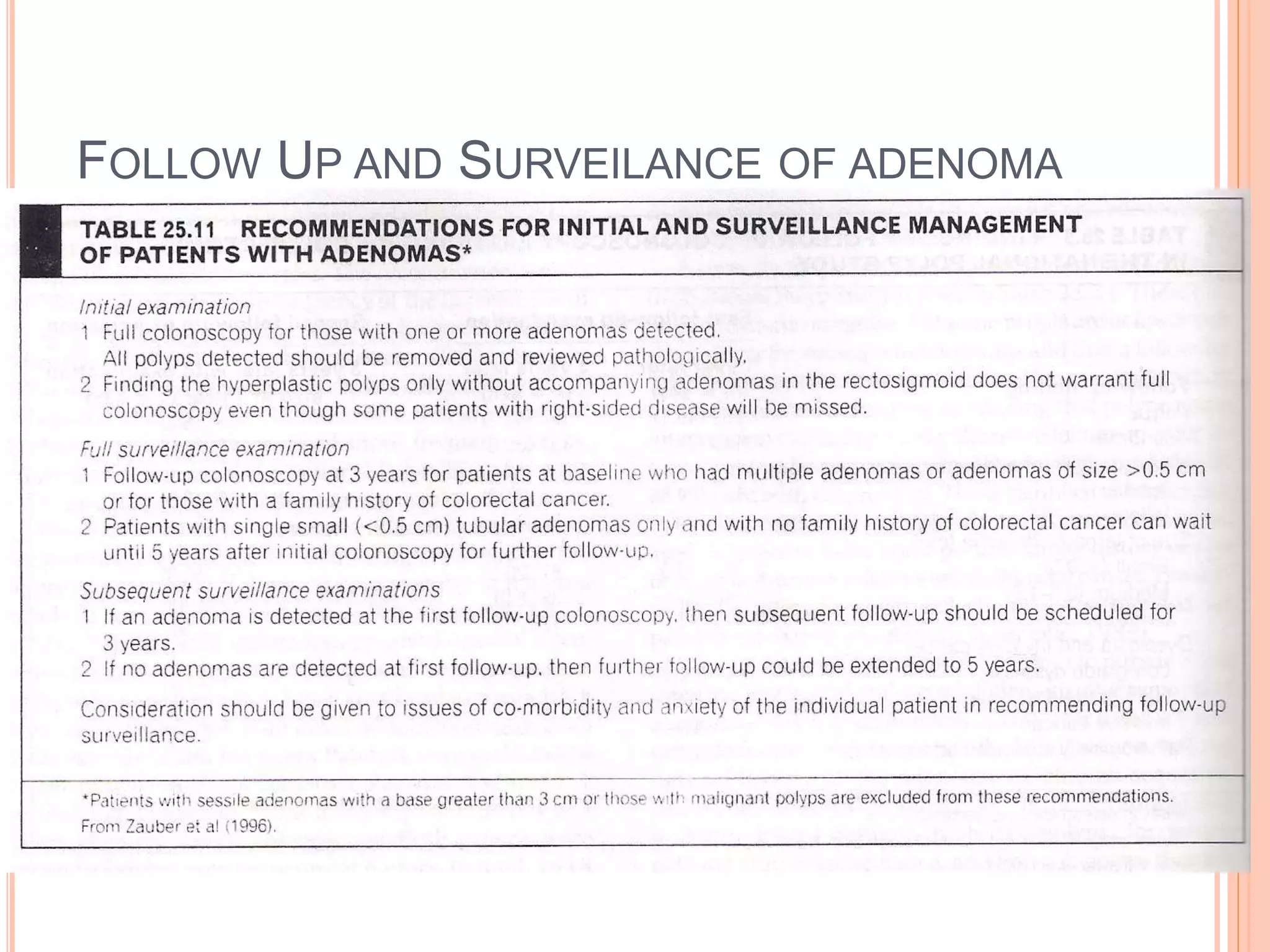
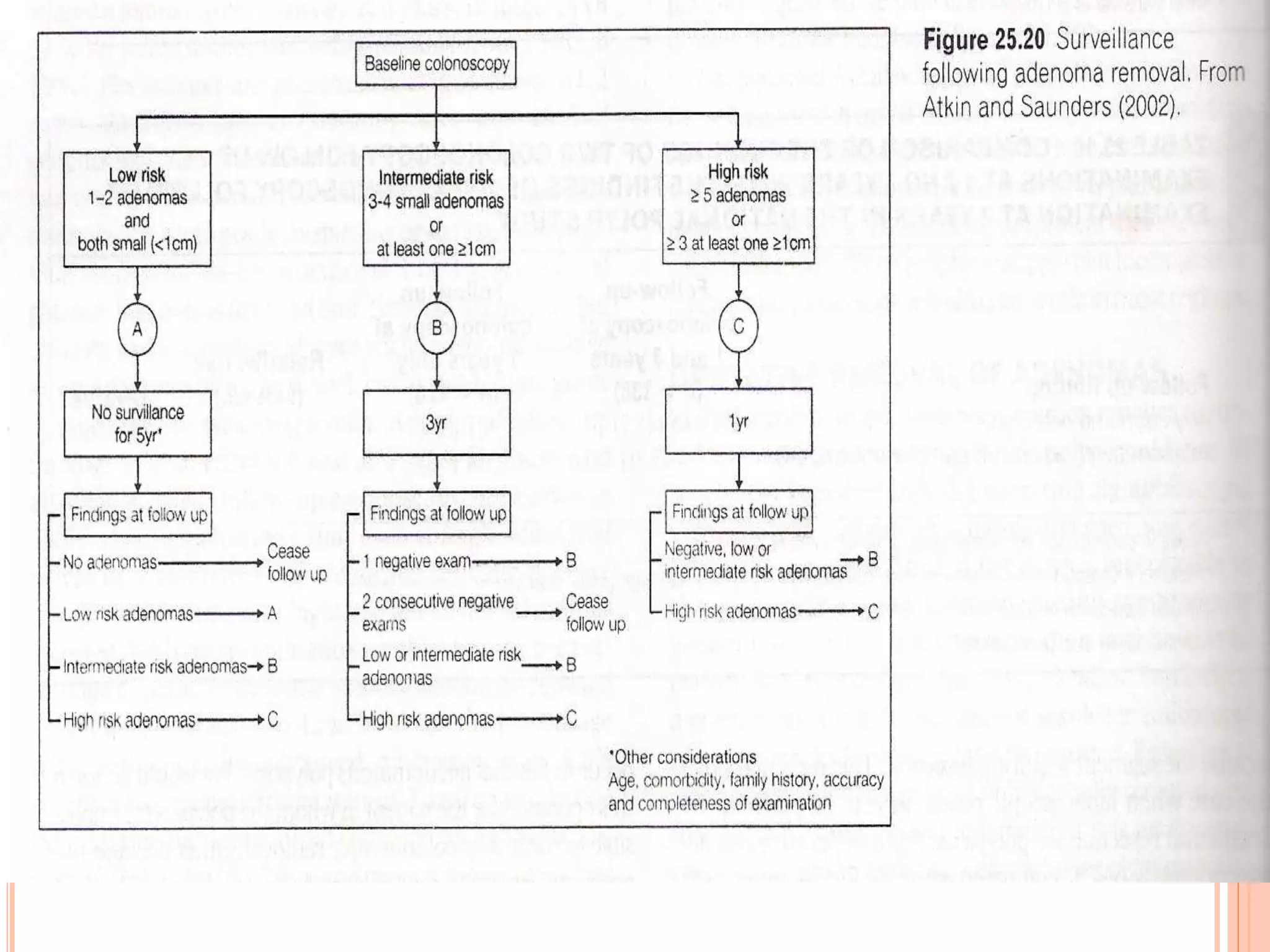

This document discusses benign neoplasms of the colon and rectum. It defines benign neoplasms and provides classifications of polyps, including non-neoplastic polyps like hyperplastic, hamartomatous, and inflammatory polyps. It also discusses neoplastic polyps, specifically adenomas, providing details on different types (tubular, tubulovillous, villous), sizes (early, intermediate, late), and characteristics. The document outlines approaches to diagnosis including examinations, tests, and instruments. It covers treatment methods like polypectomy and complications. It concludes with recommendations for follow up and surveillance of adenomas.













































































