PRESENTER : MODERATOR:
DrShreeraksha KS Dr Basavaraj Y
2nd year general surgery PG Assistant Professor
Dept of General Surgery, GIMS Dept of General Surgery, GIMS
LOWER LIMB AMPUTATIONS
2.
Anatomy
• Regions oflower limb
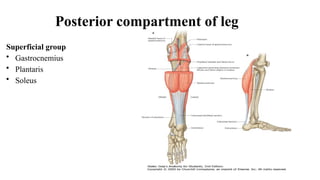
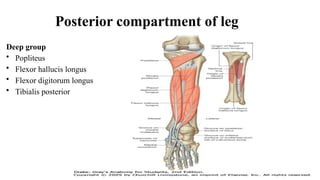
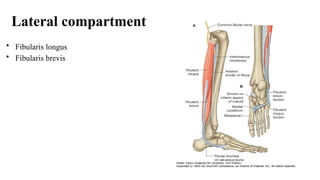
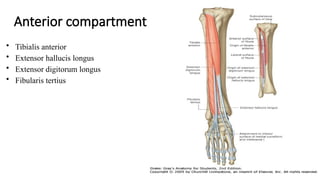
• Muscles and compartments
• Arterial supply
• Venous drainage
3.
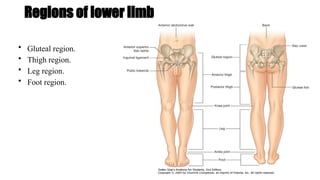
Regions of lowerlimb
• Gluteal region.
• Thigh region.
• Leg region.
• Foot region.
4.
Bones
• Gluteal region
-Pelvic bone
- Femur
• Thigh
- Femur
- Patella
• Leg region
- Tibia
- Fibula
• Foot
- Tarsal
- Metatarsal
- Phalanges
5.
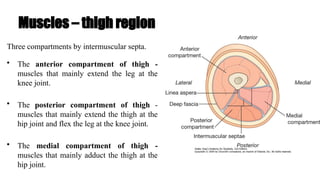
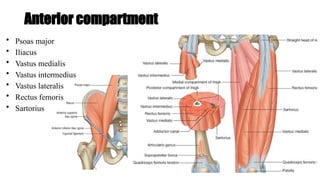
Muscles – thighregion
Three compartments by intermuscular septa.
• The anterior compartment of thigh -
muscles that mainly extend the leg at the
knee joint.
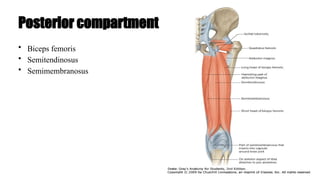
• The posterior compartment of thigh -
muscles that mainly extend the thigh at the
hip joint and flex the leg at the knee joint.
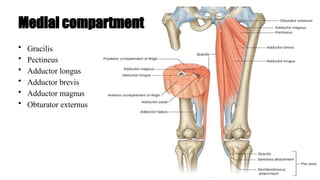
• The medial compartment of thigh -
muscles that mainly adduct the thigh at the
hip joint.
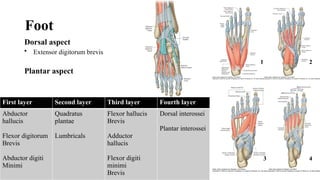
Foot
Dorsal aspect
• Extensordigitorum brevis
Plantar aspect
First layer Second layer Third layer Fourth layer
Abductor
hallucis
Flexor digitorum
Brevis
Abductor digiti
Minimi
Quadratus
plantae
Lumbricals
Flexor hallucis
Brevis
Adductor
hallucis
Flexor digiti
minimi
Brevis
Dorsal interossei
Plantar interossei
1 2
3 4
15.
DEFINITION
Part of thelimb is removed through one or more bones.
“Amputation” derived from the Latin word “amputare” (to excise, to cut out).
16.
HISTORY
• Amputation waspracticed from the time of Neanderthals mostly as a form of
punishment rather than for treatment.
• Early surgical amputation was a crude procedure by which a limb was rapidly
severed from an unanesthetized patient. The open stump was crushed or dipped in
boiling oil to obtain hemostasis.
• Olden days amputation was a procedure done for leprosy and ergotism
• In World War I and II amputations were commonly done procedures along with
invention of prosthesis.
TYPES OF AMPUTATION
•End bearing/ cone bearing: weight taken up by the body
• Non end bearing/ side bearing: weight taken up by the joint
• weight bearing / non weight bearing
• Provisional / Guillotine / Formal
• Open / Closed
23.
• OPEN AMPUTATION:
Theskin is not closed over the amputation stump
usually when the wound is not healthy.
Procedures for constructing a satisfactory stump:
a) Secondary closure: Closure of skin flaps after a few days.
b) Plastic repair: Soft tissues are repaired without cutting the bone and skin flaps
are closed.
c) Revision of the stump: Terminal granulation tissue and scar tissue, as well as a
moderate amount of bone is removed and the stump reconstructed.
d) Re-amputation.
'OPTIMUM LEVELS FORAMPUTATION’
• In thigh, the optimum length is 25 to 30 cm (10-12 inches) from the tip of the
greater trochanter. The shortest length should be 10 cm (4 inches).
• In leg, the optimum length is 14 cm (5 inches). The minimum length should be
7.5 cm (3 inches).
• Factors to be considered :
• Length of the stump – as long as possible.
• Wound healing
28.
Local factors helpingfor determining the level of amputation.
Physical examination – skin colour, hair growth, skin temperature
Investigations-
• Arteriogram,
• Skin perfusion tests –
– Laser doppler flometry,
– Thermography,
– Tissue uptake of intravenous fluorescein,
– Tissue clearance of intradermally injected xenon – 133,
– Transcutaneous oxygen measurement
29.
THE IDEAL STUMP
•heal adequately by 1st intention.
• rounded, gentle contour, with adequate padding.
• sufficient length to bear prosthesis.
• thin scar which does not interfere with prosthetic function.
• adequate adjacent joint movement.
• adequate blood supply.
• Scar should be in a place where it is not exposed to pressure.
• Scar should be freely mobile over underlying tissues.
30.
• Skin andscar should be freely mobile over the underlying bone. It is achieved
only if deep fascia is closed properly.
• Scar and skin should be free to achieve free movement of the prosthesis.
• Socket of the prosthesis with mobile skin creates a piston to bone to move like a
joint.
• Skin should not be unfolded.
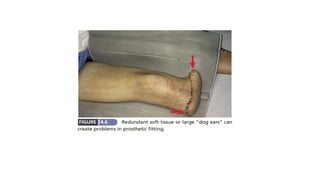
• Redundant soft tissue should not be there. Stump should be free from tenderness
and conical
32.
PRINCIPLES – FORCLOSED TYPE
• Tourniquet: Use of a tourniquet is highly desirable except in case of an ischaemic
limb, diabetic foot with calcified arteries
• Ex-sanguination: Usually a limb should be squeezed (ex-sanguinated) by wrapping it
with a stretchable bandage (Esmarch bandage) before a tourniquet is inflated. It is
contraindicated in cases of infection and malignancy for fear of spread of the same
proximally.
• Skin flaps: The skin over the stump should be mobile and normally sensitive, but
atypical skin flaps are preferable to amputation at a more proximal level.
33.
• Muscles:
• Myoplasty– Suturing of muscle to the periosteum or the fascia of opposing
musculature.
• Myodesis - Suturing of muscle or tendon to bone. (Contraindicated in peripheral
vascular diseases).
• Nerves : gently pulled distally into the wound, and divided with a sharp knife so
that the cut end retracts well proximal to the level of bone section.
• Large nerves such as the sciatic nerve contain relatively large vessels and should
be ligated before they are divided.
34.
• Major bloodvessels : Isolated and doubly ligated using non-absorbable sutures.
The tourniquet to be released before skin closure and meticulous haemostasis to
be secured.
• Bone level : Excessive periosteal stripping proximally may lead to the
formation of 'ring sequestrum' from the end of the bone.
Bony prominences which are not well padded by soft tissues should be resected.
Sharp edges of the cut bone should be made smooth.
• Drain: A corrugated rubber drain should be used for 48-72 hours post-
operatively.
35.
Evaluation of patientswho need amputation
• Hematocrit, anemia correction, transfusion of blood
• Control of infection with Antibiotics
• Decision of level of amputation by skin temperature, arterial doppler
• Informed consent
• Plan for prosthesis and rehabilitation by physiotherpaist and rehabilitation team
36.
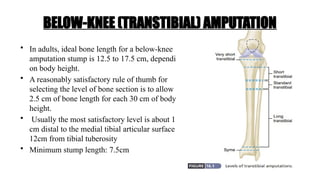
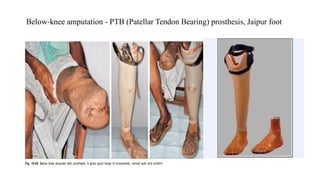
• In adults,ideal bone length for a below-knee
amputation stump is 12.5 to 17.5 cm, depending
on body height.
• A reasonably satisfactory rule of thumb for
selecting the level of bone section is to allow
2.5 cm of bone length for each 30 cm of body
height.
• Usually the most satisfactory level is about 15
cm distal to the medial tibial articular surface /
12cm from tibial tuberosity
• Minimum stump length: 7.5cm
BELOW-KNEE (TRANSTIBIAL) AMPUTATION
37.
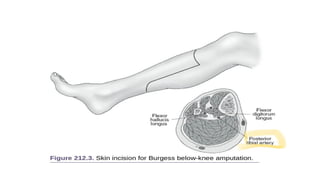
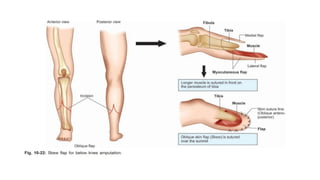
• The longposterior flap - length 1.5 times the diameter of the leg.
• The anterior flap is cut down to bone at the level of bone division.
• Elevation of the anterior flap of skin and muscle off the underlying bone is kept to a
minimum, and 1 cm is adequate.
• The tibia is then divided and bevelled anteriorly.
• The fibula is divided 1 cm more proximally.
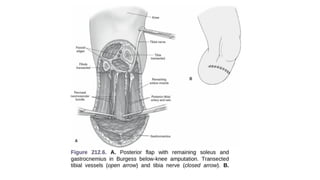
• The posterior flap should retain deep fascia and some underlying muscle throughout
its length in order to safeguard skin perfusion. However, the muscle bulk must be
reduced to obtain a tapered stump.
39.
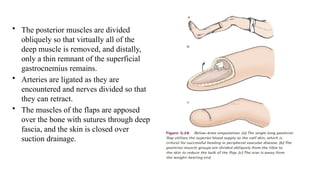
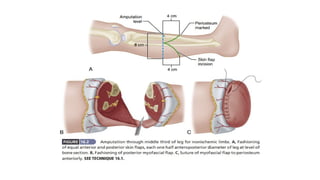
• The posteriormuscles are divided
obliquely so that virtually all of the
deep muscle is removed, and distally,
only a thin remnant of the superficial
gastrocnemius remains.
• Arteries are ligated as they are
encountered and nerves divided so that
they can retract.
• The muscles of the flaps are apposed
over the bone with sutures through deep
fascia, and the skin is closed over
suction drainage.
42.
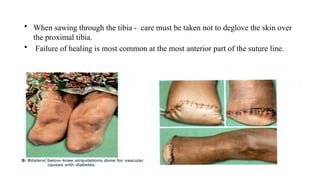
• When sawingthrough the tibia - care must be taken not to deglove the skin over
the proximal tibia.
• Failure of healing is most common at the most anterior part of the suture line.
43.
VARIATIONS OF THESTANDARD METHOD
A ‘SKEW’ FLAP TECHNIQUE :
Skin and muscle flaps are fashioned separately.
Equal skin flaps are based on the blood supply of the skin, which is anatomically
related to the venous drainage of the long and short saphenous veins, and relies on
collateral vessels running with the sural and saphenous nerves.
A single posterior muscle flap is used.
46.
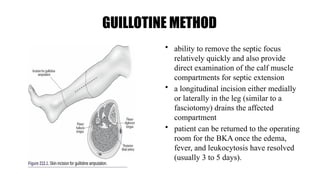
GUILLOTINE METHOD
• abilityto remove the septic focus
relatively quickly and also provide
direct examination of the calf muscle
compartments for septic extension
• a longitudinal incision either medially
or laterally in the leg (similar to a
fasciotomy) drains the affected
compartment
• patient can be returned to the operating
room for the BKA once the edema,
fever, and leukocytosis have resolved
(usually 3 to 5 days).
47.
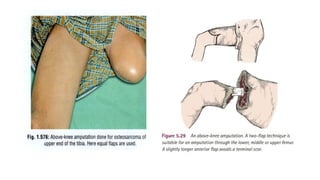
ABOVE-KNEE (TRANSFEMORAL) AMPUTATIONS
commonamputations for :
• ischemia and trauma.
• patient will be unable to heal a BKA
• unlikely to mobilize after an amputation
• significant knee contracture
48.
• The longerthe stump the better the control of the prosthesis, and ideally 70 percent
of the femur (or around 25–30 cm as measured from the tip of the greater trochanter)
should be retained.
• In a child the whole femur to be preserved.
• The underlying pathology sometimes dictates an amputation in the upper third of the
femur, but if < 10 cm of femur can be preserved, then disarticulation through the hip
joint to be preferred in a younger patient in order to fit a more satisfactory prosthesis.
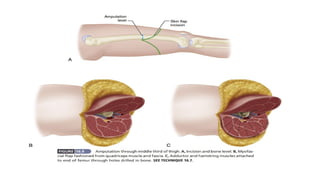
50.
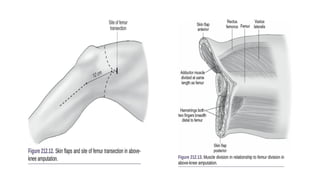
• Equal anteriorand posterior myocutaneous flaps
• point of femoral shaft transection 12 cm from the knee joint
∼
• The circumference of the extremity should be estimated at this point, and the
intersection of the anterior and posterior flaps should be one half of this.
• distal aspect of the flaps should then extend to a distance two fingerbreadths
proximal to the patella
• The quadriceps muscle is sutured to the hamstrings - muscle action on the stump
remains balanced.
• In a younger patient some form of more formal myodesis should be carried out.
53.
RAY AMPUTATION (TRANSMETATARSALTOE
AMPUTATION)
• Amputation of toe with removal of head of metatarsal
• Preoperative assurance of adequate circulation
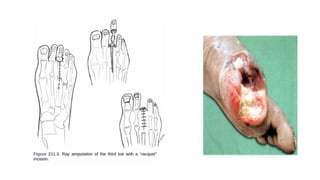
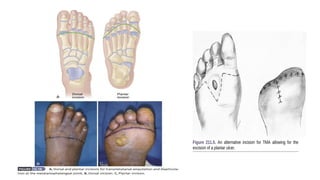
• racquet-type longitudinal incision
• A ratio of incision length to width of at least 3:1 will aid primary closure
• In vascular cases, forefoot sepsis, the wound is left open
55.
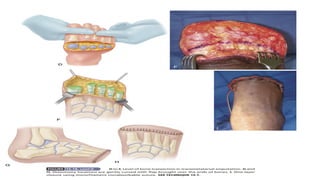
• After removingthe head of the metatarsal, the foot is then assessed for ascending
infection. In compressing the foot if pus is noted along the extensor or flexor
tendons, these compartments are opened for more aggressive drainage.
• In the case of a first-ray amputation, the incision is made as two curvilinear lines on
both the dorsum and plantar surfaces of the foot, extending down to the level of the
bone, exposing the metatarsal head - sacrifice FHL
• Full weight bearing should be avoided until wound healing has occurred, generally
about a month
56.
TRANSMETATARSAL (GILLIE’S) AMPUTATION
•Allows patients to ambulate with a shoe filler and steel shank with rocker soles
but without a prosthesis.
• Limb length is preserved, and gait is maintained well.
• Heals less predictably than transtibial amputations.
• Indication - infection or gangrene involving multiple digits and possibly some of
the dorsal skin proximal to the metatarsophalangeal joints.
59.
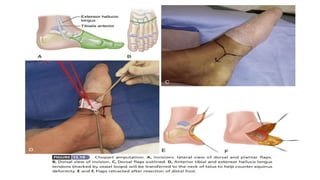
CHOPART (MIDTARSAL) AMPUTATION
•talonavicular joint and calcaneocuboid joints are disarticulated
• only talus and calcaneum are preserved
• limb is immobilized for 6 weeks after surgery with ankle in neutral position.
• Equinovarus deformity is the problem
62.
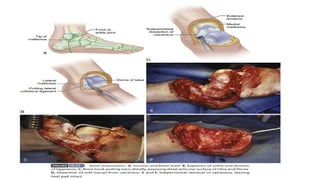
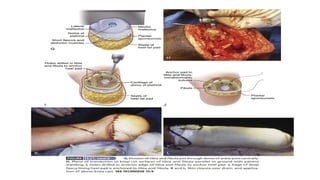
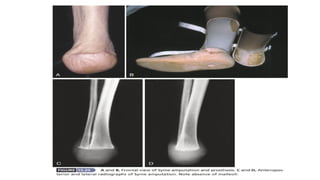
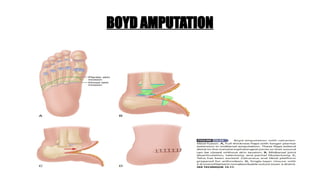
SYME’S AMPUTATION
• Aclassical ankle amputation.
• Removal of the foot with calcaneum and cutting of tibia and fibula just above the
ankle joint with retaining heel flap
• produces a durable weight-bearing stump.
• Used in trauma (crush injury), congenital deformities of foot wherein amputation is
inevitable, nonischaemic damage of foot and malignancies in distal part of the foot.
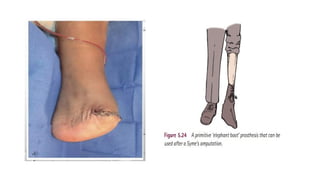
• Special value to patients who do not have access to modern artificial limbs.
• The end of the stump is at a height of about 6–8 cm from the ground and may be
walked on without a prosthesis
63.
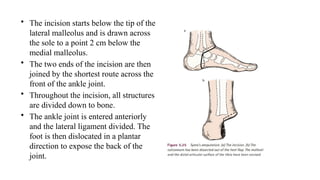
• The incisionstarts below the tip of the
lateral malleolus and is drawn across
the sole to a point 2 cm below the
medial malleolus.
• The two ends of the incision are then
joined by the shortest route across the
front of the ankle joint.
• Throughout the incision, all structures
are divided down to bone.
• The ankle joint is entered anteriorly
and the lateral ligament divided. The
foot is then dislocated in a plantar
direction to expose the back of the
joint.
POST-OPERATIVE PERIOD
• Physiotherapyas advised.
• Regular dressings are done.
• Crutch is used initially, after 3 months prosthesis is placed.
• Rehabilitation.
71.
COMPLICATIONS OF AMPUTATION
•EARLY :
a) Haemorrhage.
b) Haematoma :
Inadequate haemostasis, loosening of the ligature and inadequate wound drainage
are the common causes.
Haematoma - delayed wound healing and infection
72.
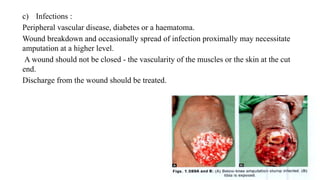
c) Infections :
Peripheralvascular disease, diabetes or a haematoma.
Wound breakdown and occasionally spread of infection proximally may necessitate
amputation at a higher level.
A wound should not be closed - the vascularity of the muscles or the skin at the cut
end.
Discharge from the wound should be treated.
73.
LATE COMPLICATIONS
• Pain.
•Ulceration of stump.
• Ring sequestrum formation.
• Flap necrosis.
• Painful scar.
• Phantom limb
74.
Stump pain: COMMON
•infection, poor blood supply, causalgia, stump neuroma, phantom limb, DVT,
formation of spurs and osteophytes, adherant scar
Skin flap necrosis: COMMON
A minor or major skin flap necrosis - insufficient circulation of the skin flap, infection,
hematoma, inadequate flap length causing stretching
Small areas of flap necrosis - excised, may heel with dressings
Larger areas - laying open, redesigningof the flaps / revision of stump
75.
Phantom limb:
• Awarenessof sensation as if the amputated part is still present.
• Severe pain at the amputated part just prior to amputation maling brain area
• Most prominent in the period immediately following amputation, and gradually
diminishes with time.
• Reassurance, prosthesis, analgesia
• Prevention by pain control 24h before amputation
76.
Stump neuroma:
• Failureof cutting the nerve proximal to level of bone division
• Proliferation of nerve fibrils
• Analgesics, reassurance, prosthesis
• Re exploration with excision of end neuroma
77.
Ulceration over stump:
•Due to necrosis, infection, lengthy bone stump pressing flap, prosthesis, pooor
nutrition, DM, ischemia
• Small ulcer - regular dressigns, suturing
• Large ulcer - flap to cover defect
Contracture of the joint:
• Improper positioning of the amputation stump, leading to contractures.
• A mild or moderate contracture - appropriate positioning and gentle passive-
stretching exercises.
• Severe deformity - surgical correction.
78.
PROSTHESIS
Substitution to apart of the body to achieve its optimum function.
TYPES :
1. Exoskeletal prosthesis.
2. Endoskeletal prosthesis with modular system.
The prosthesis does not have sensation, proprioception or muscle power. The power is
provided to a prosthesis by forces arising from movement of the residual or other side
limb – BODY POWERED PROSTHESIS.
Others - external source of power, usually rechargeable batteries used.
79.
ADVANTAGES :
• Cosmetic.
•Function of the part relatively
can be got.
• Ambulation in lower limb
prosthesis.
DISADVANTAGES :
• Infection.
• Pressure ulcers.
• Joint disability.
80.
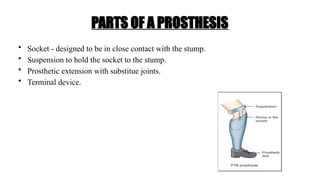
PARTS OF APROSTHESIS
• Socket - designed to be in close contact with the stump.
• Suspension to hold the socket to the stump.
• Prosthetic extension with substitue joints.
• Terminal device.
Paralympic Games
• Aperiodic series of international multisport events involving athletes with a range of
disabilities.
• Games are governed by the International Paralympic Committee (IPC).
• The Paralympics began as a small gathering of British World War II veterans in
1948.
87.
REFERENCES
• FISCHER’S MASTERYOF SURGERY 7TH
EDITION
• CAMPBELLS’S OPERATIVE ORTHOPAEDICS 14TH
EDITION.
• BAILEY AND LOVE’S SHORT PRACTISE OF SURGERY 28TH
EDITION.
• SRB's Surgical Operations Text and Atlas.
• MAHESHWARI - ESSENTIALS ORTHOPAEDICS.