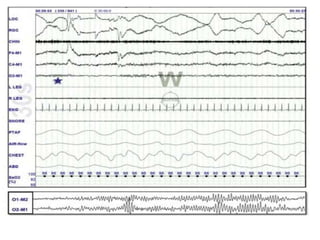
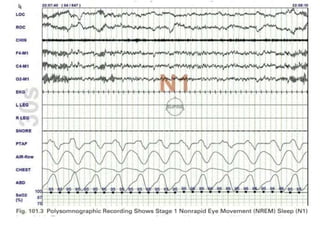
Polysomnography is a multi-parameter test used to diagnose sleep disorders. It involves the simultaneous recording of biophysiological changes that occur during sleep including brain waves, eye movements, muscle activity, heart rate, respiration, and oxygen levels. Key components measured include EEG, EOG, EMG, respiratory effort, airflow, oximetry. Together these provide information about sleep stages and identify disorders like sleep apnea, narcolepsy, restless leg syndrome. Polysomnography is performed in a sleep lab with technicians monitoring the patient overnight.




























![INDICES FOR SLEEP APNEA SYNDROMES
• Apnea-hypopnea index (AHI)
The AHI is defined as the average number of episodes of apnea
and hypopnea per hour.
• Respiratory disturbance index (RDI)
Defined as the average number of respiratory disturbances
(obstructive apneas, hypopneas, and respiratory event–related
arousals [RERAs]) per hour.](https://image.slidesharecdn.com/polysomnographypresentation-240320121946-065bd77c/85/basic-of-polysomnography-presentation-pptx-44-320.jpg)










































































