Downloaded 38 times
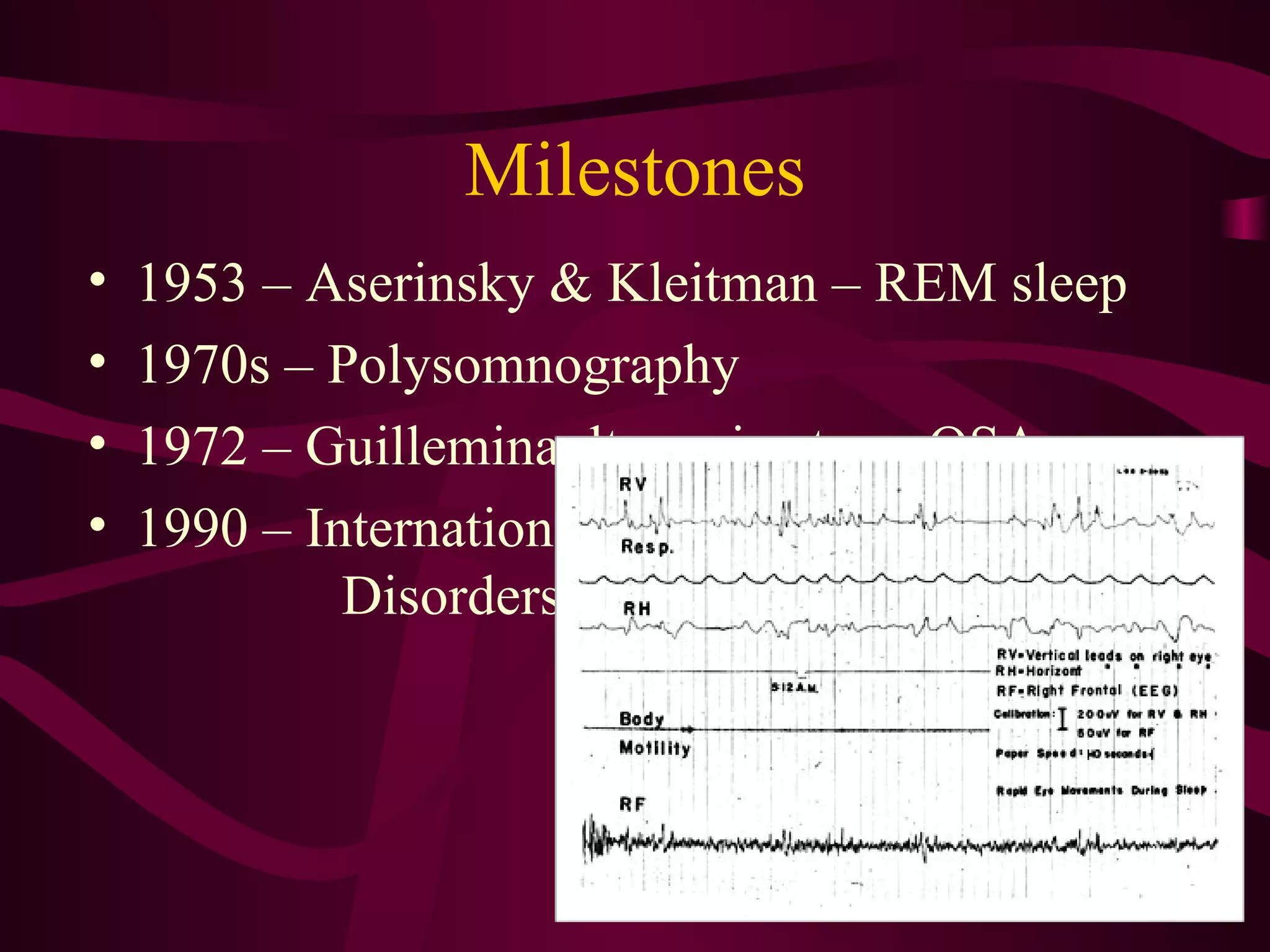
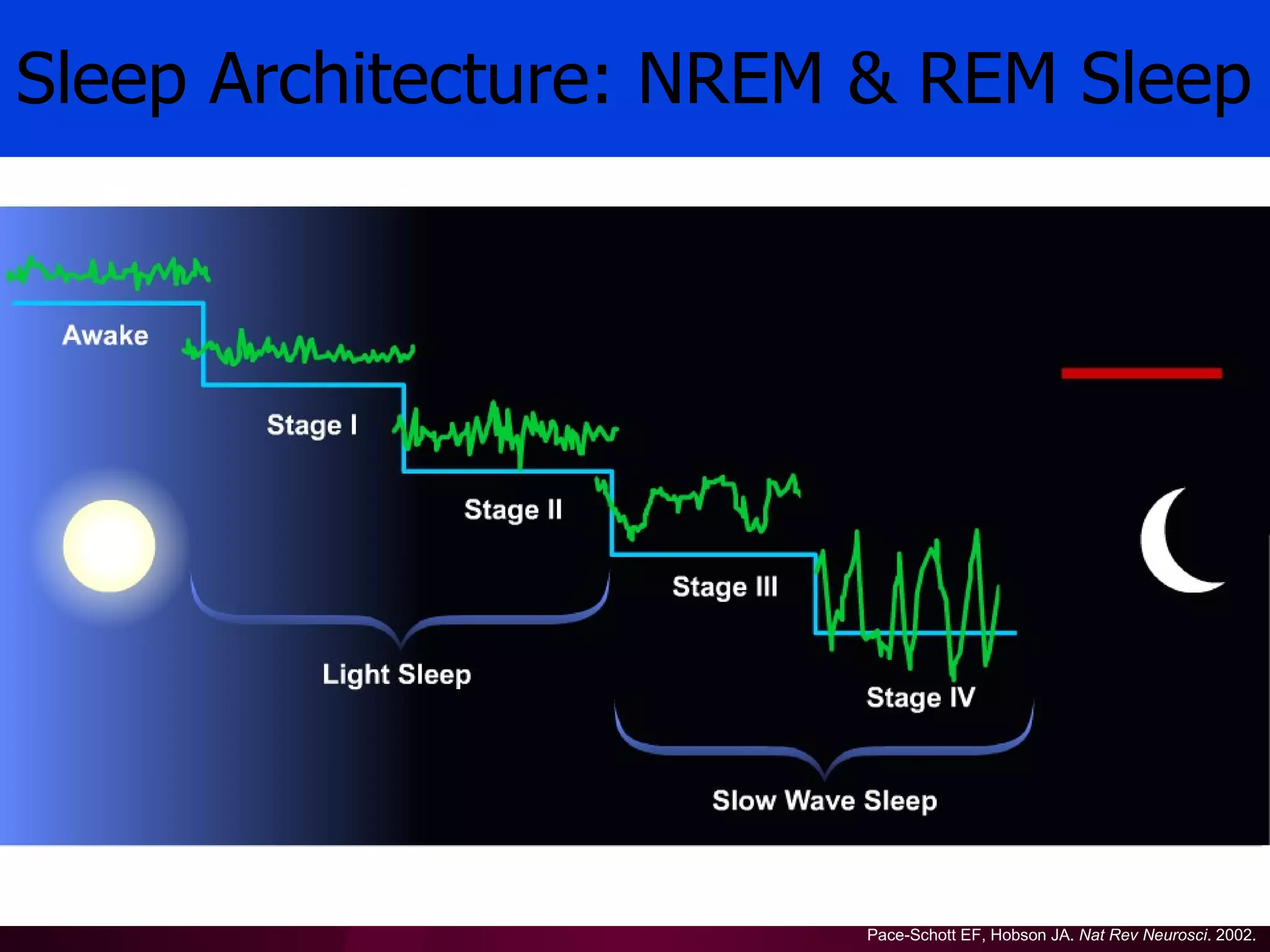
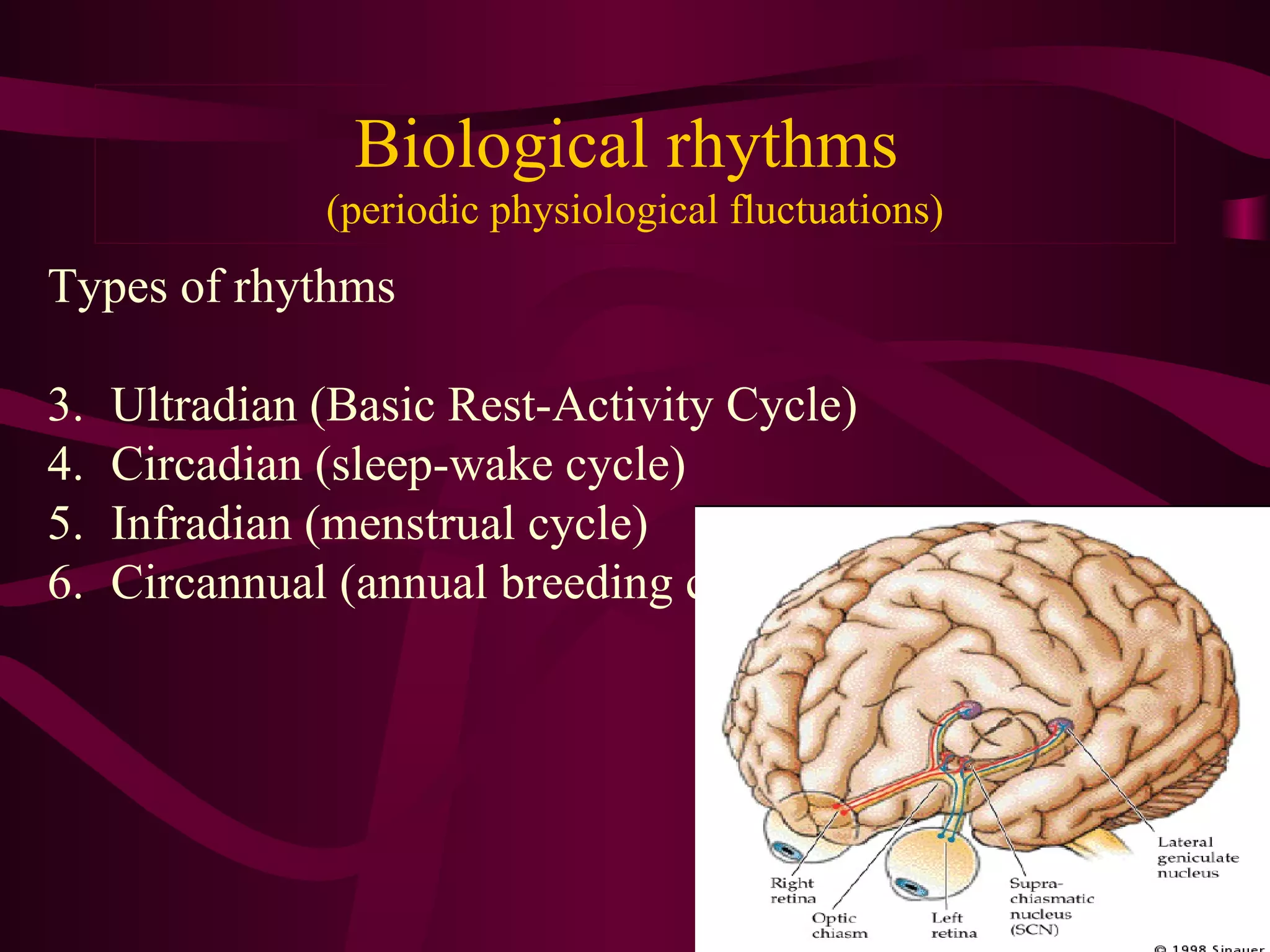
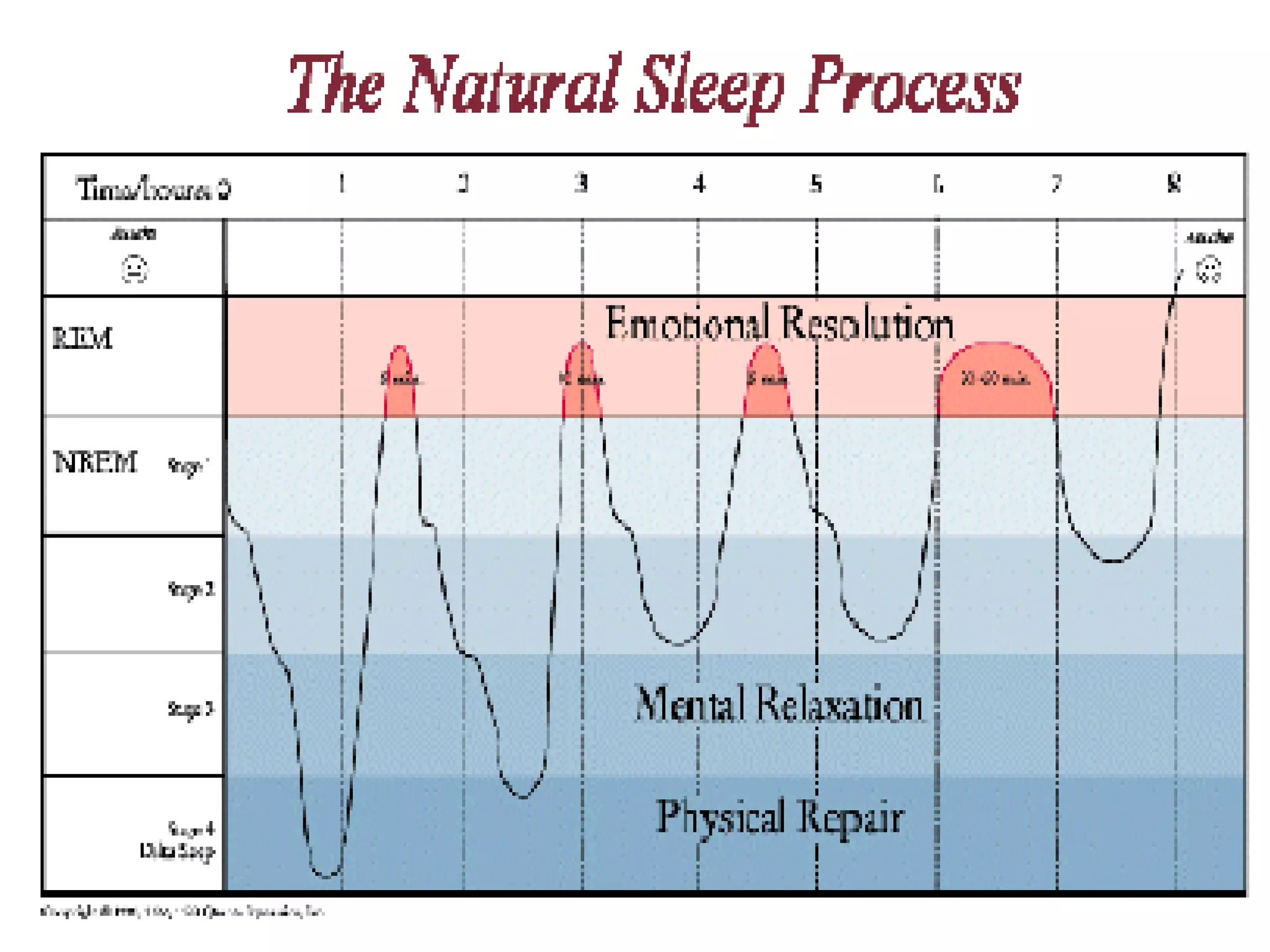
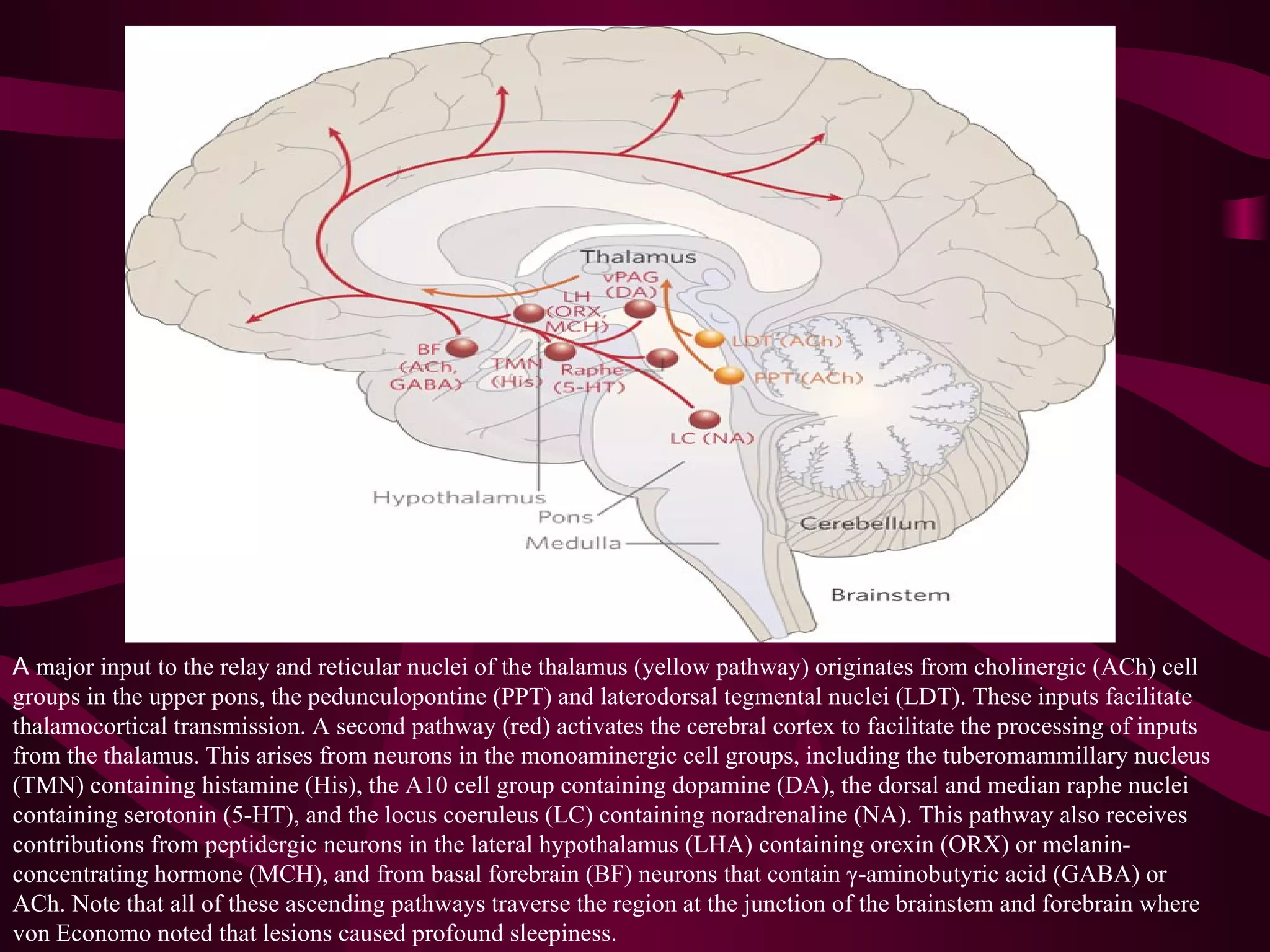
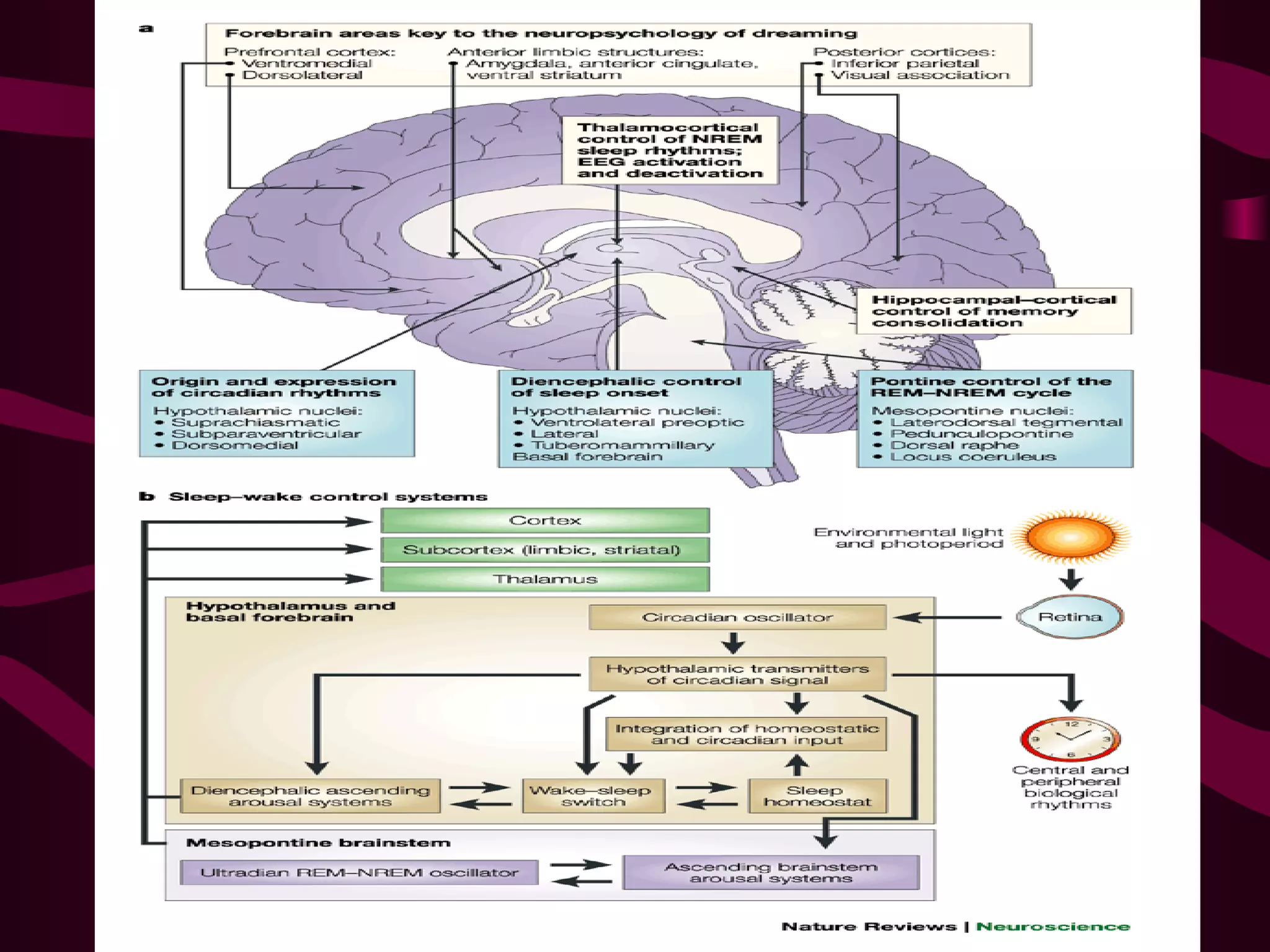
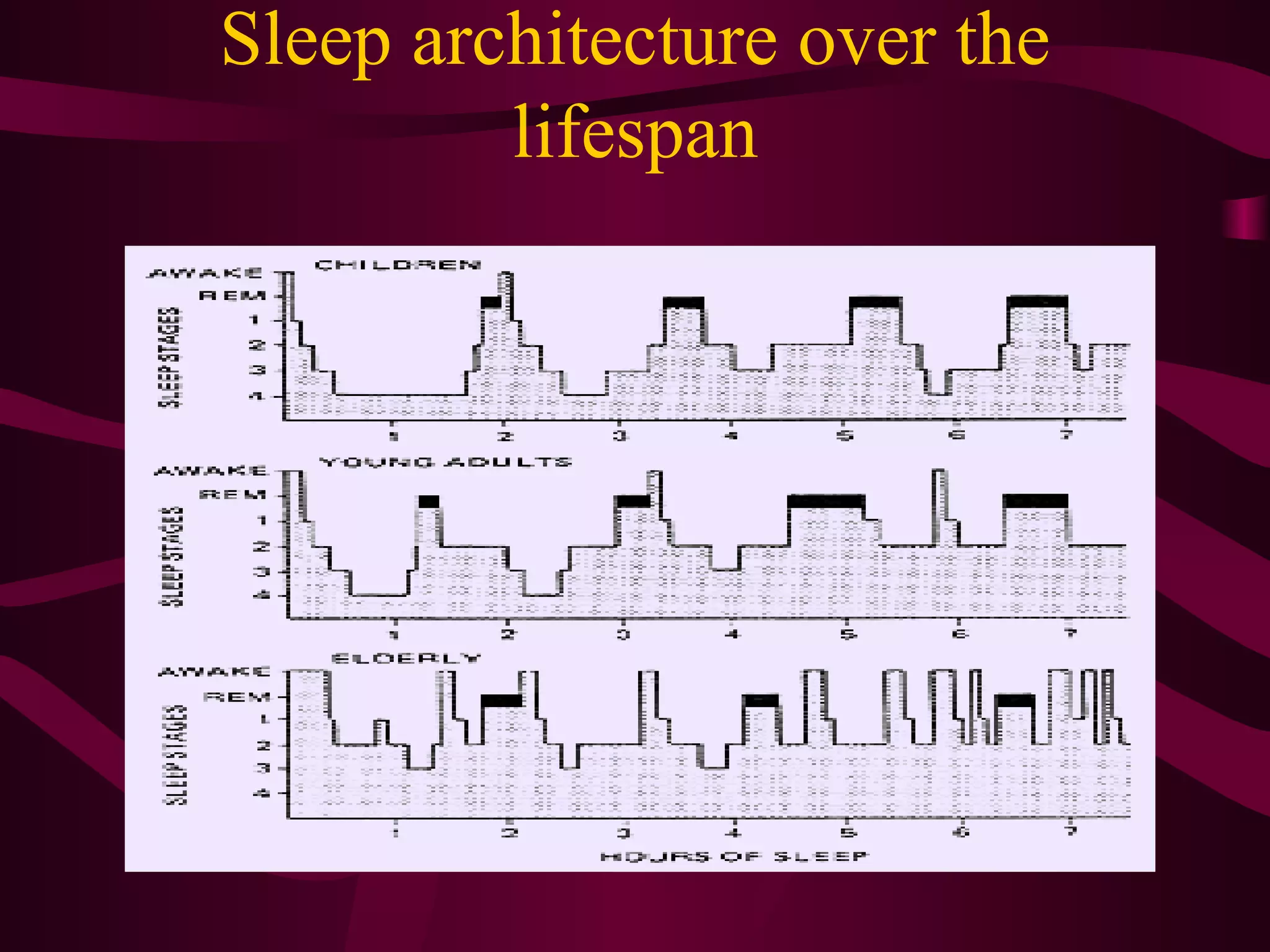
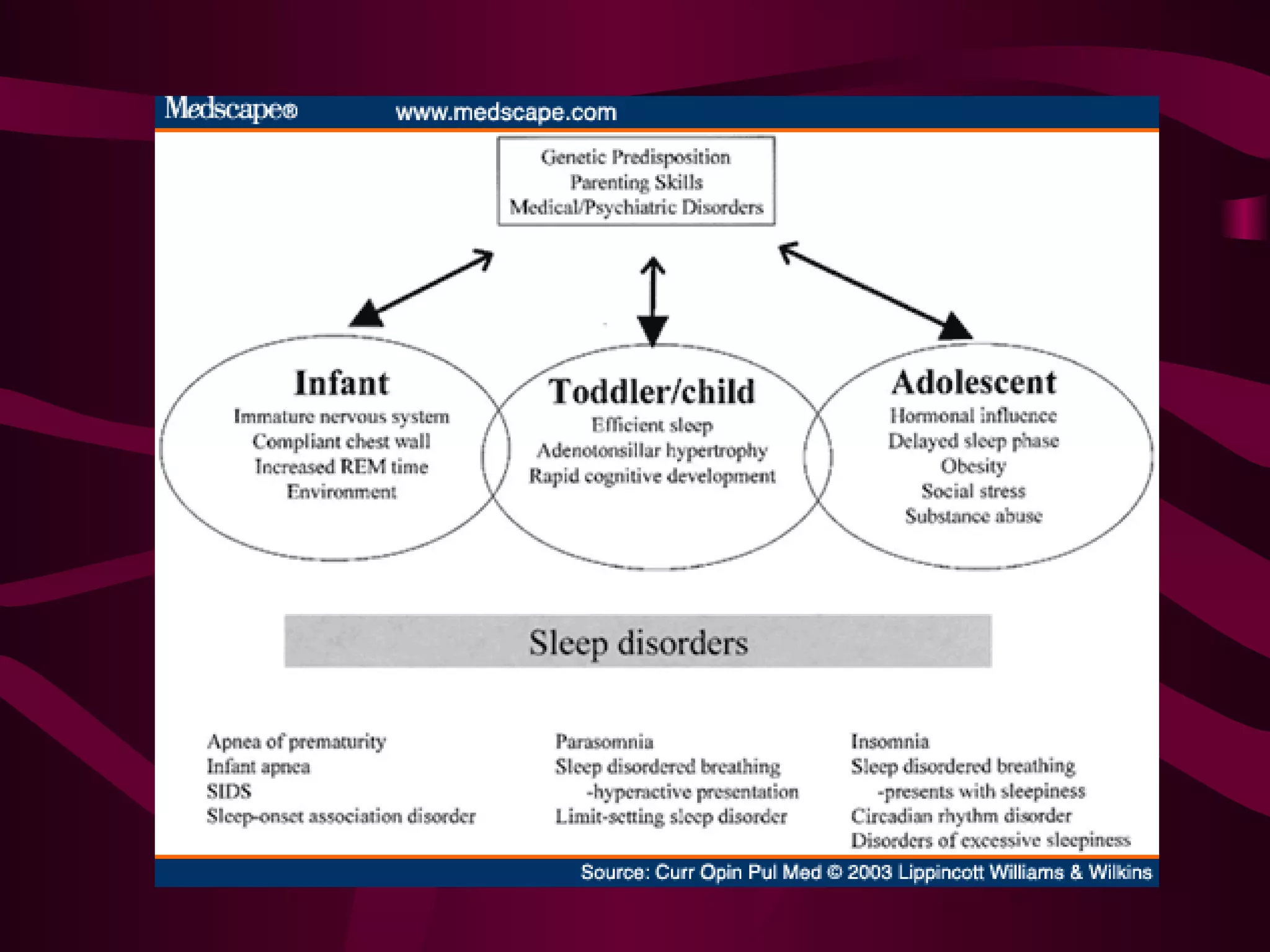
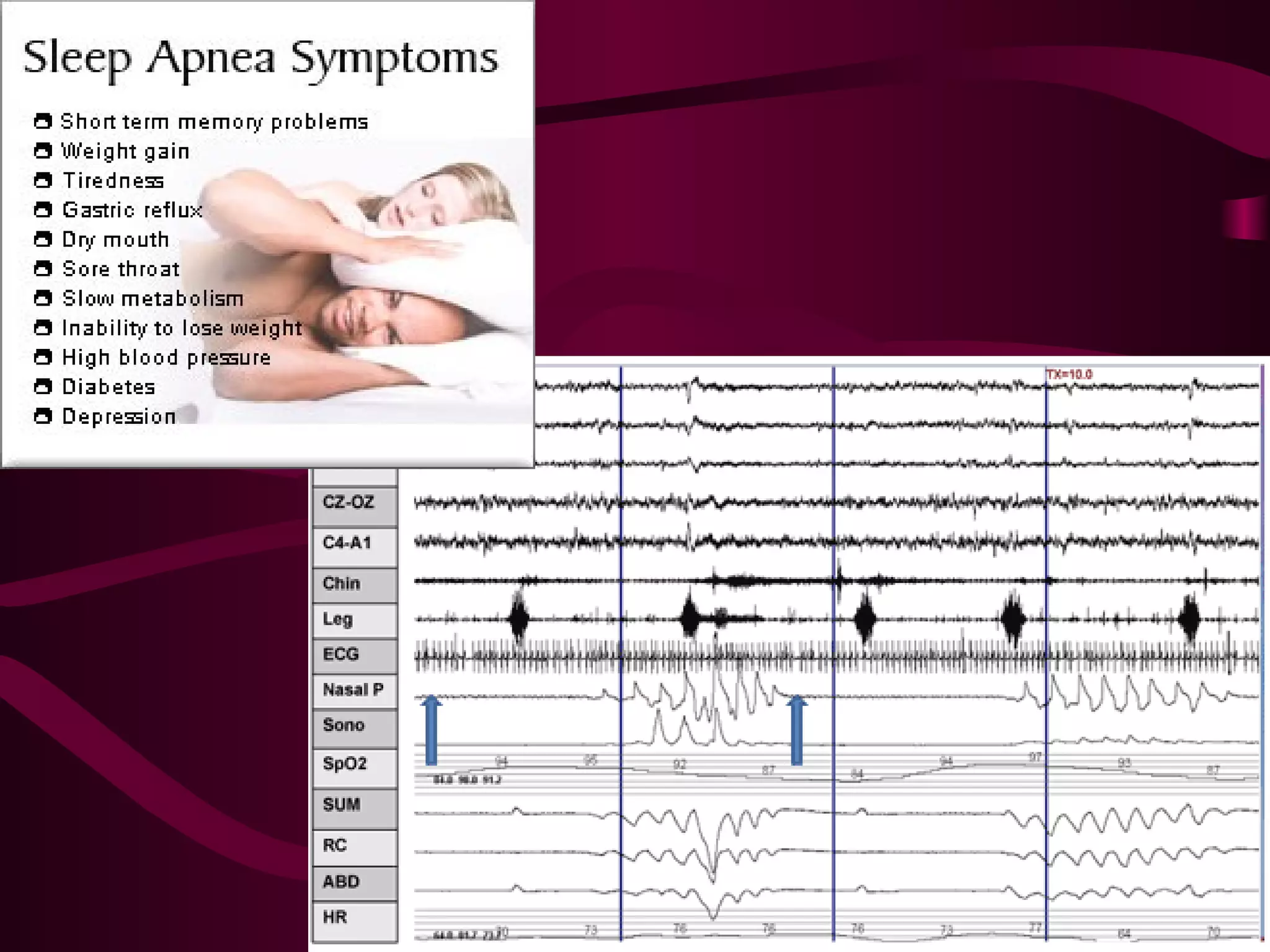
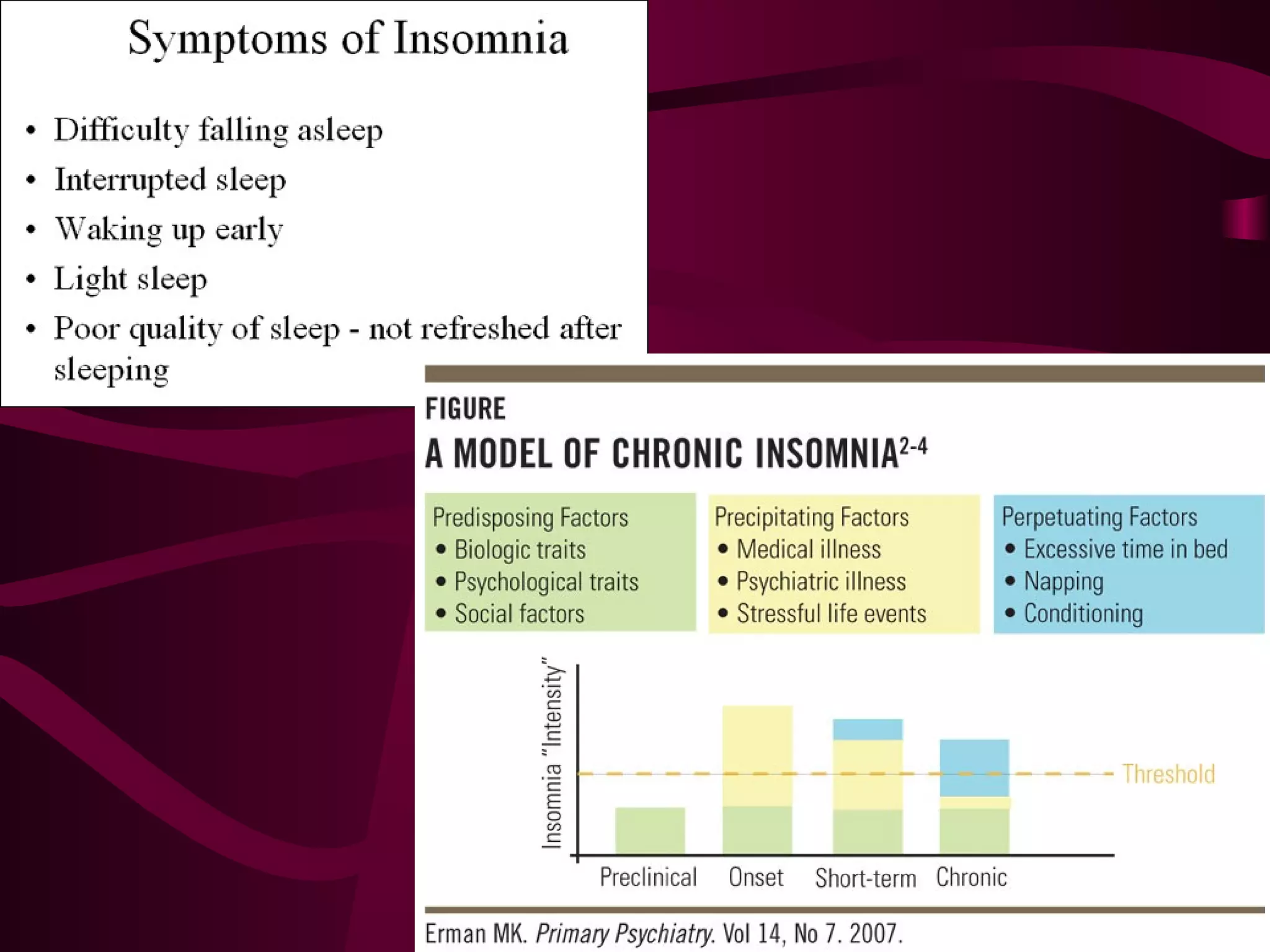
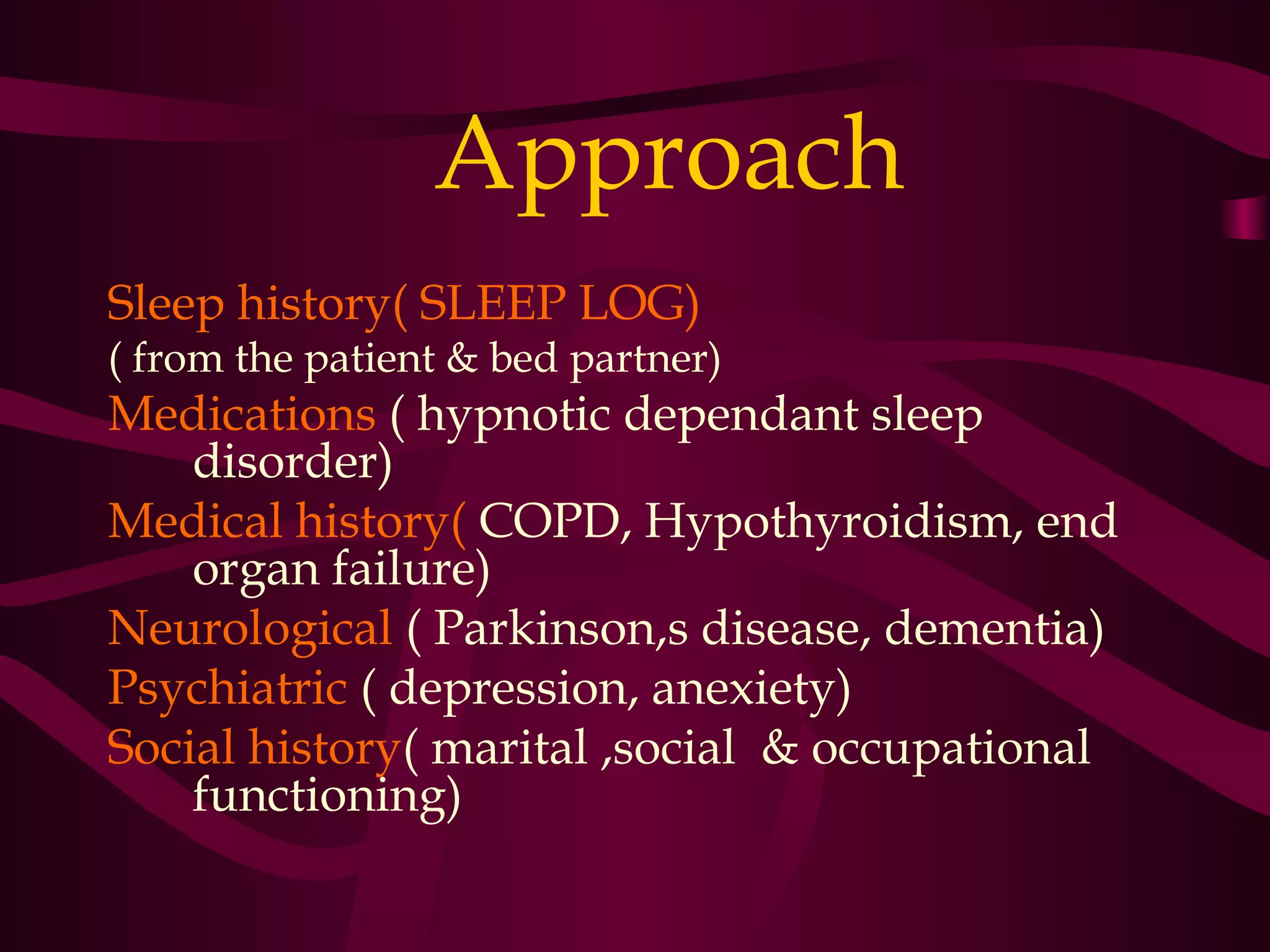
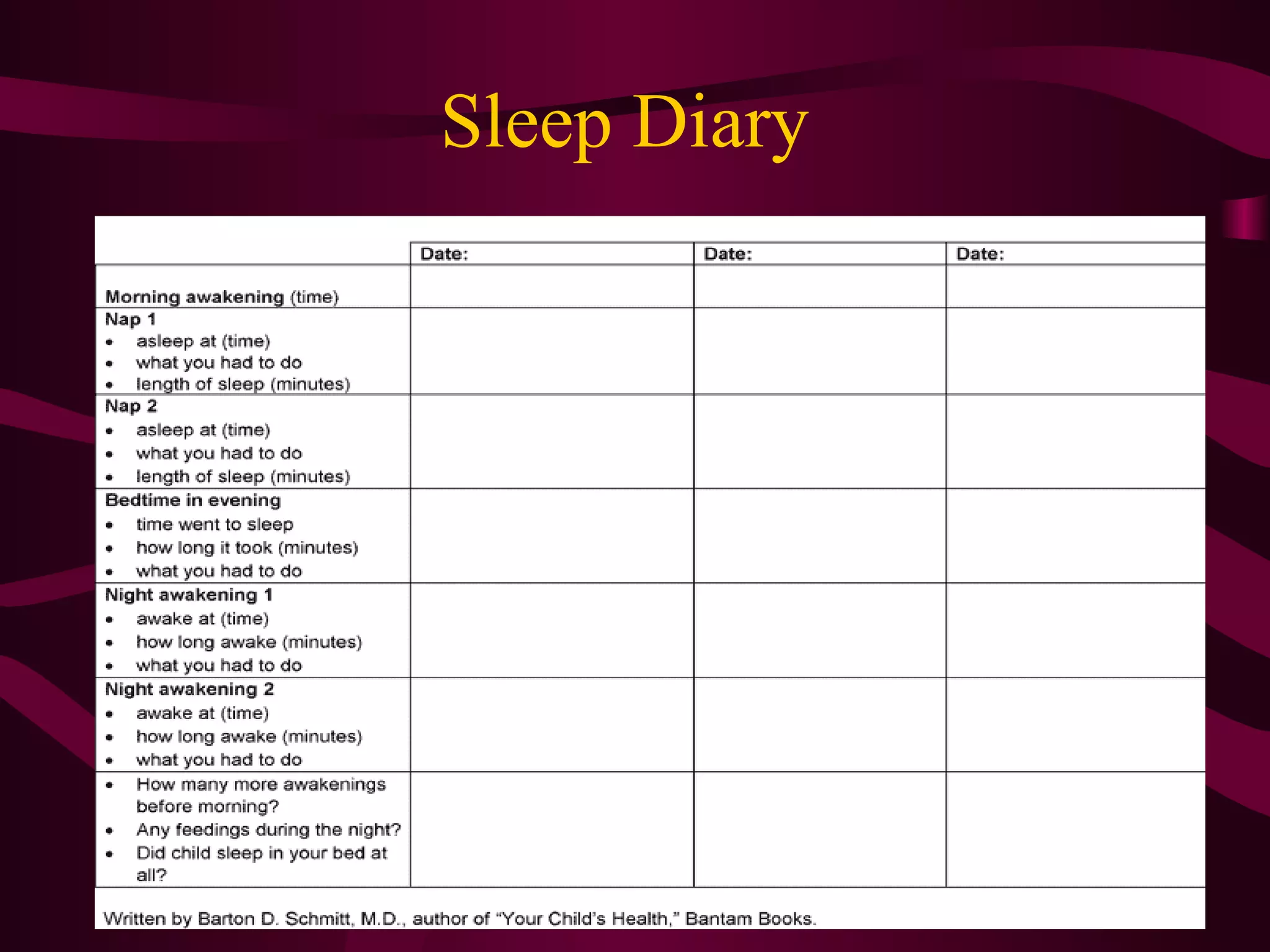
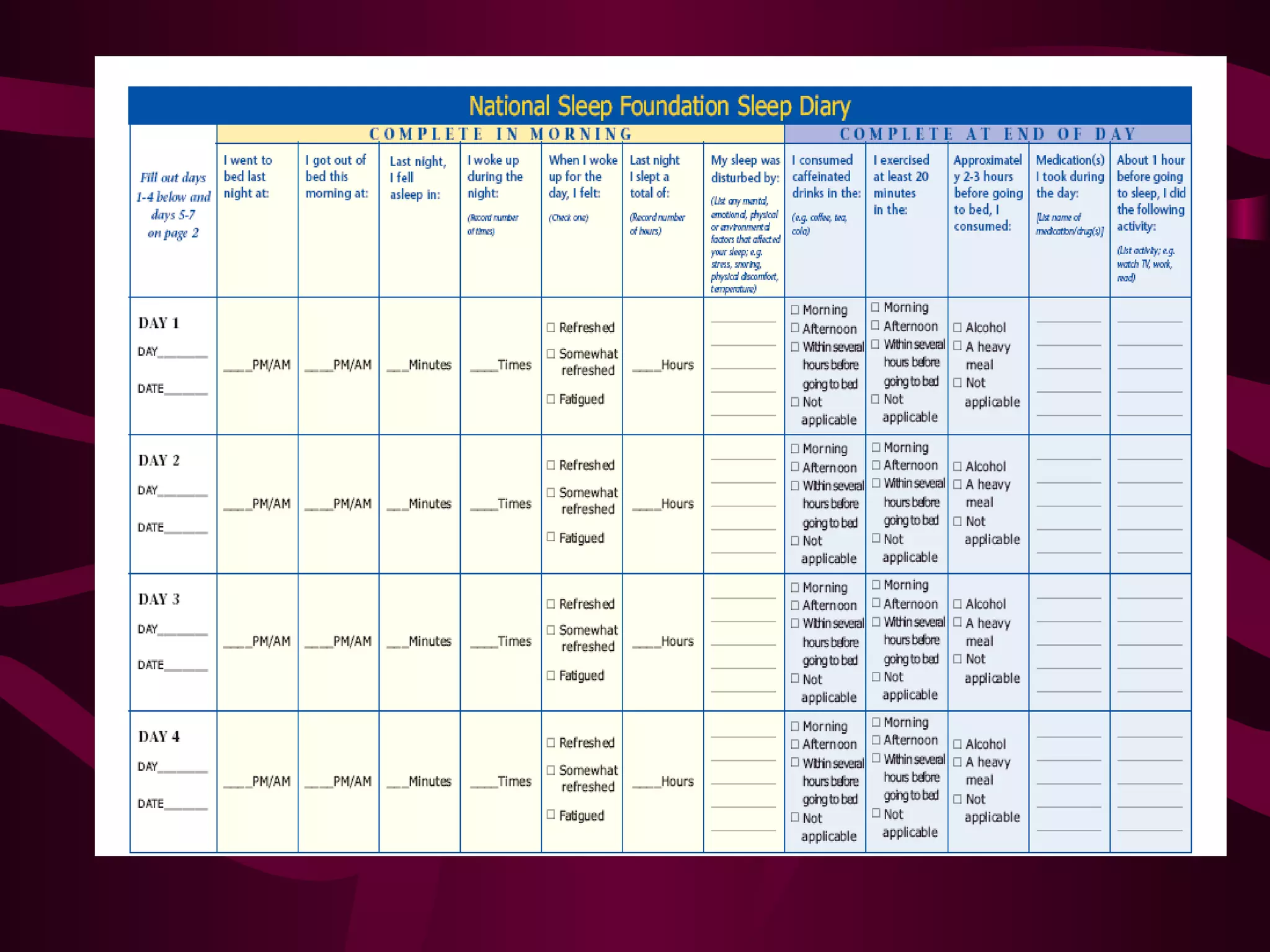
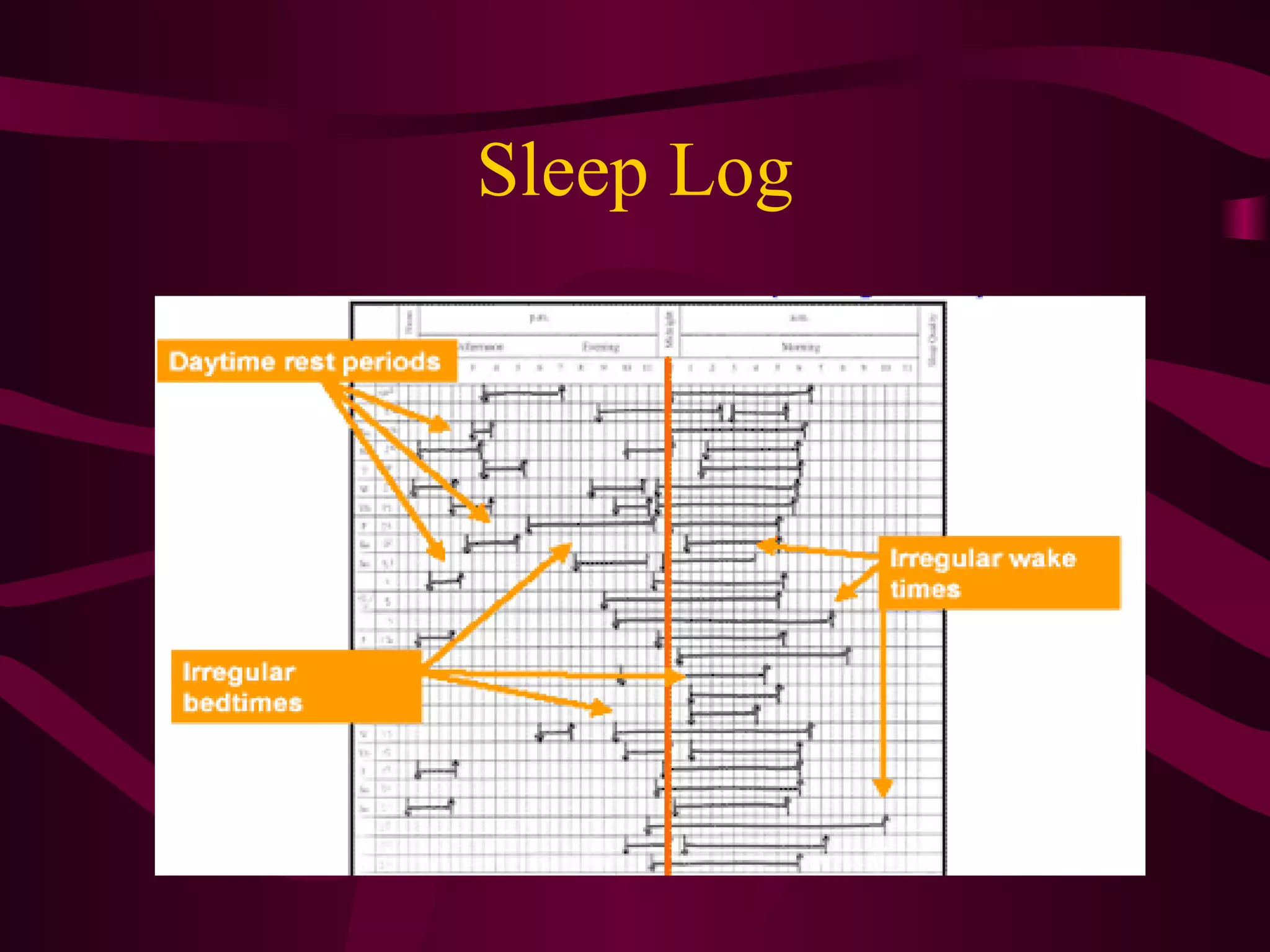
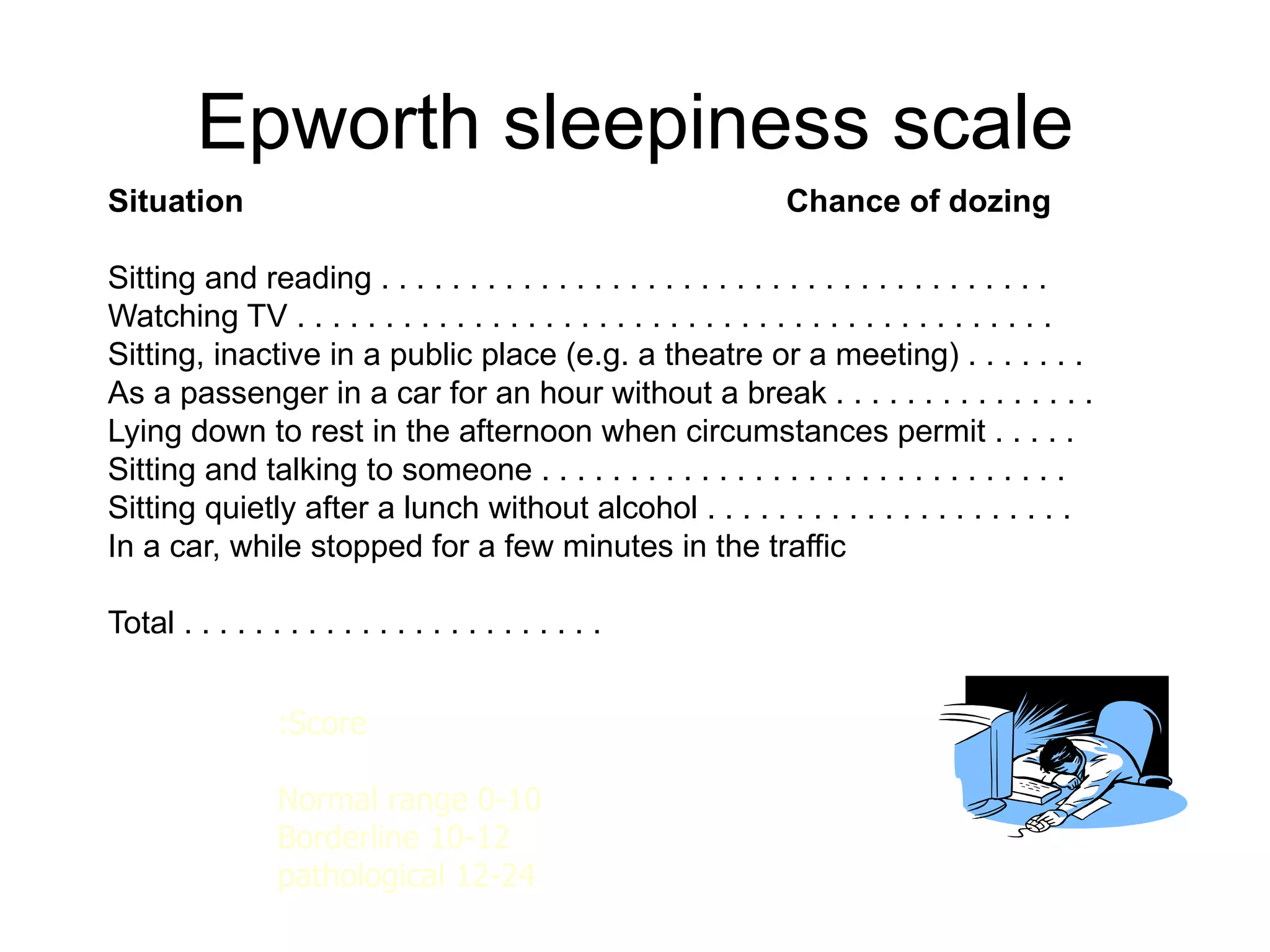
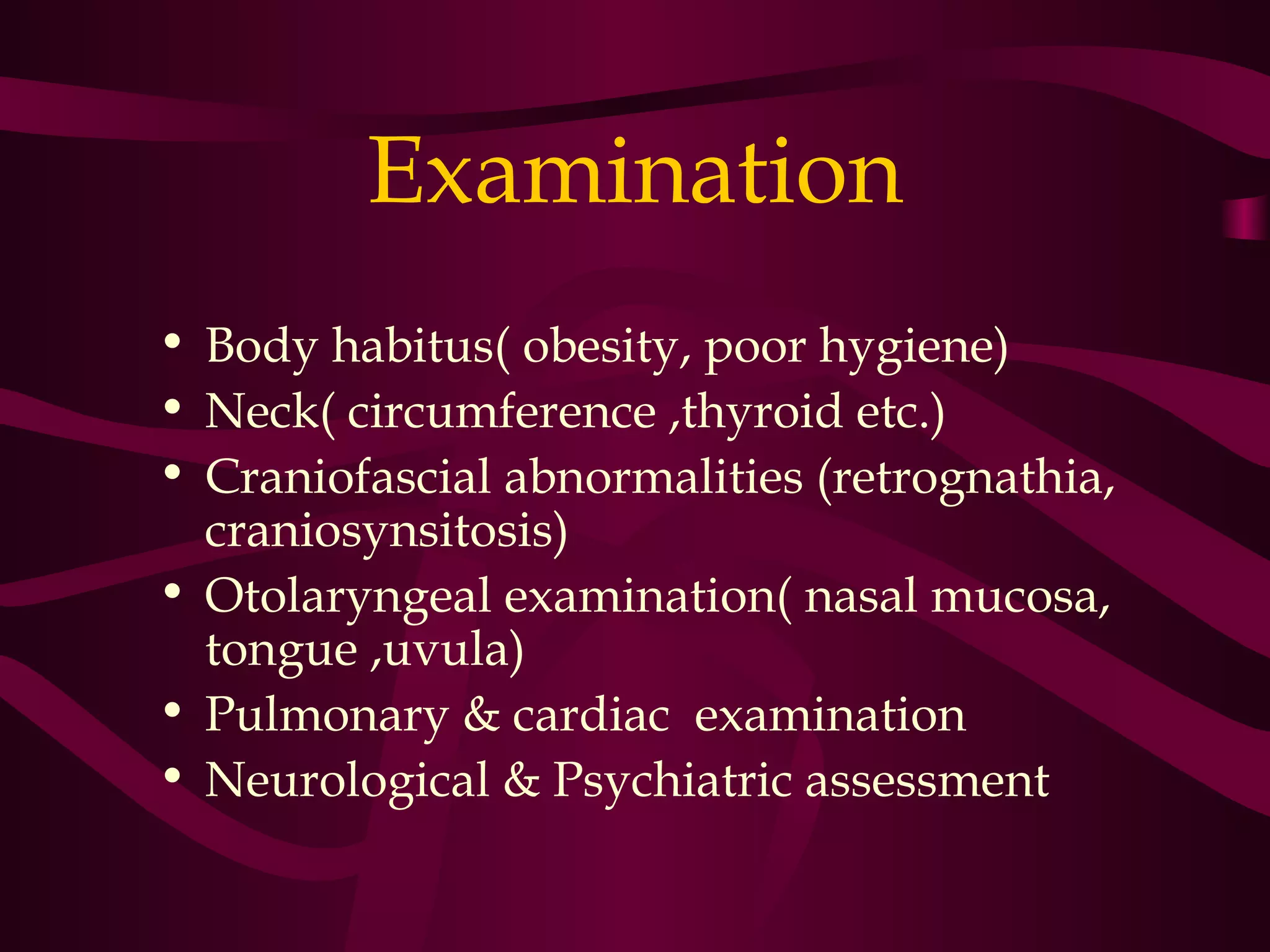
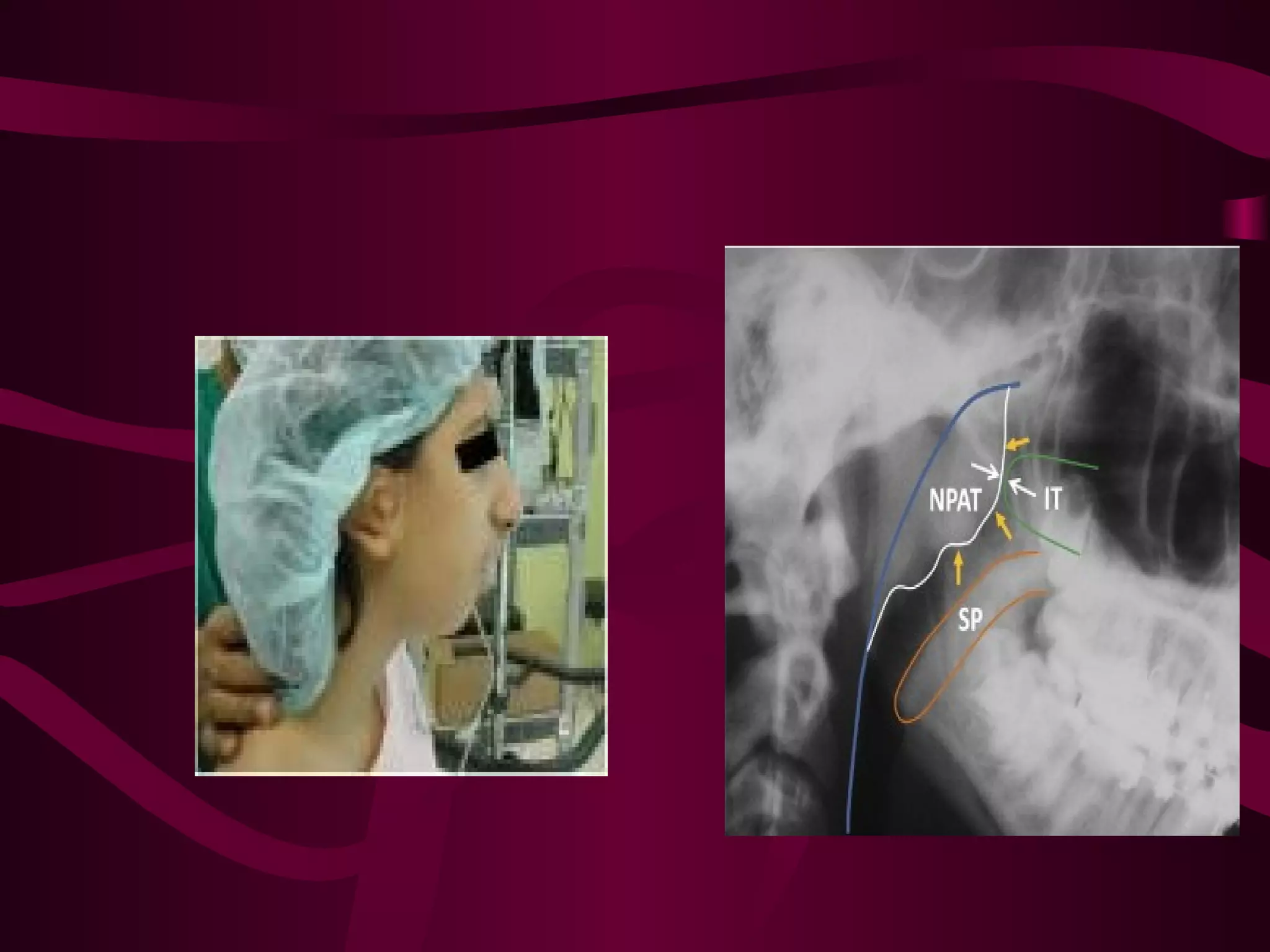
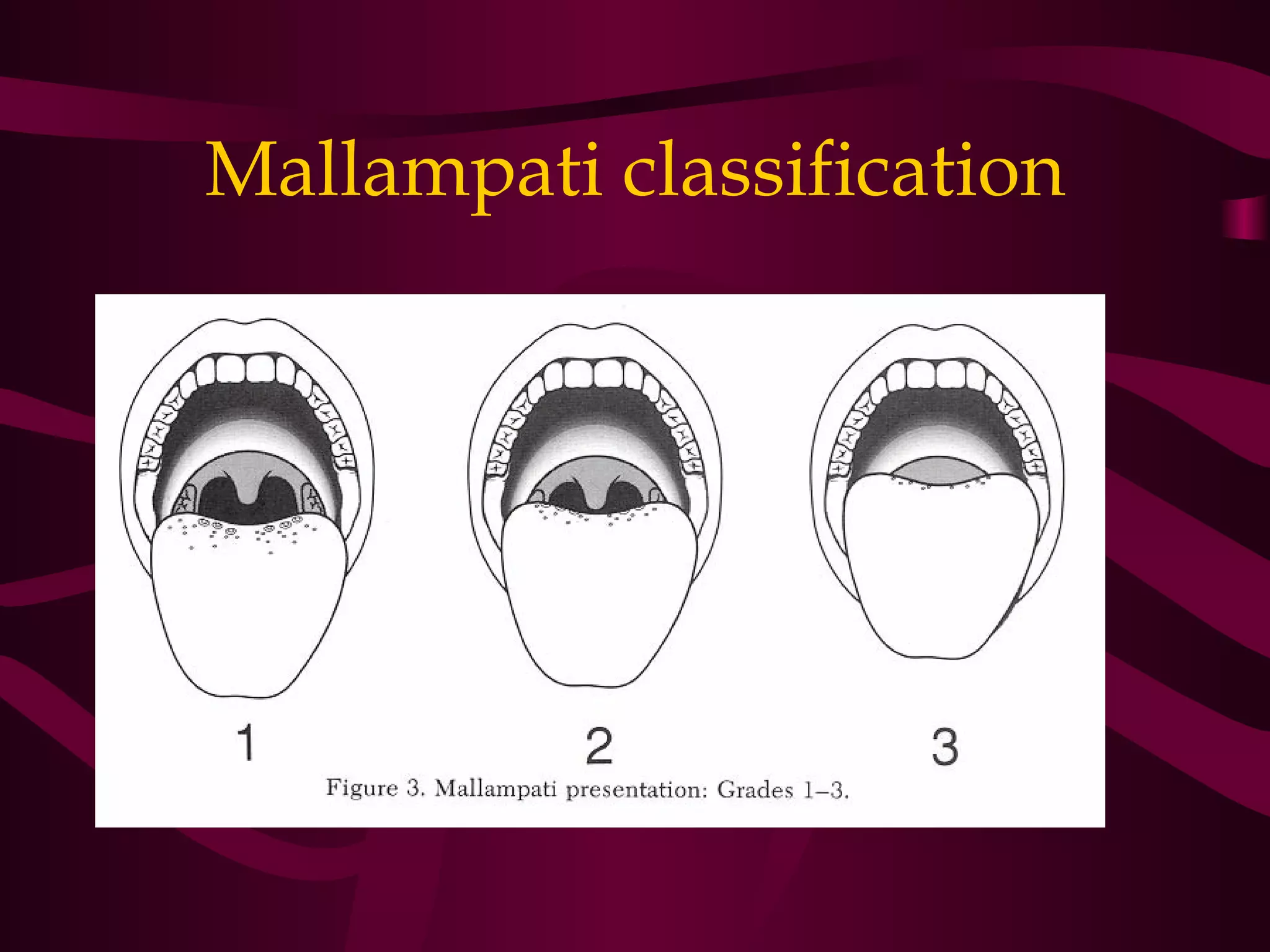
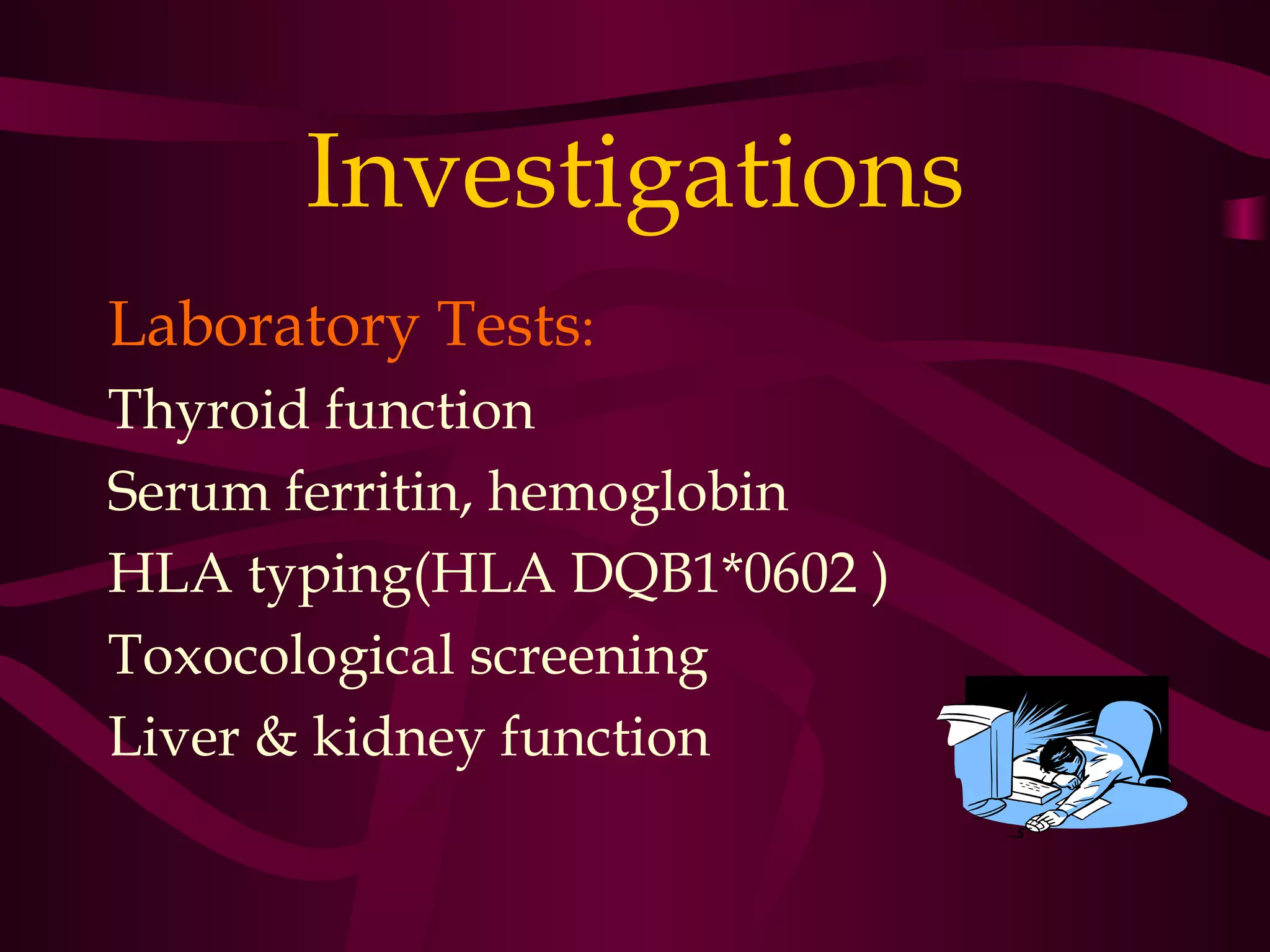

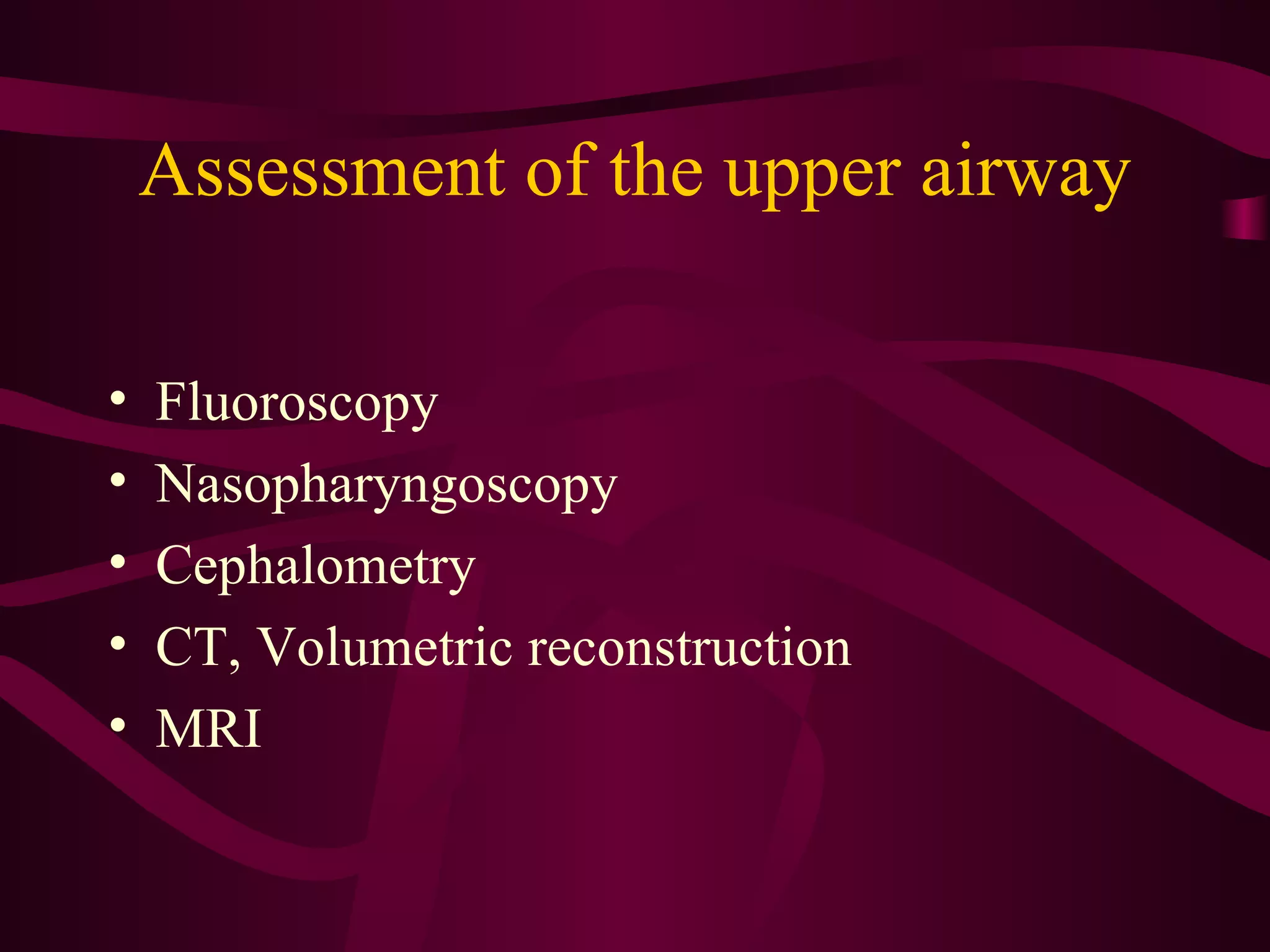
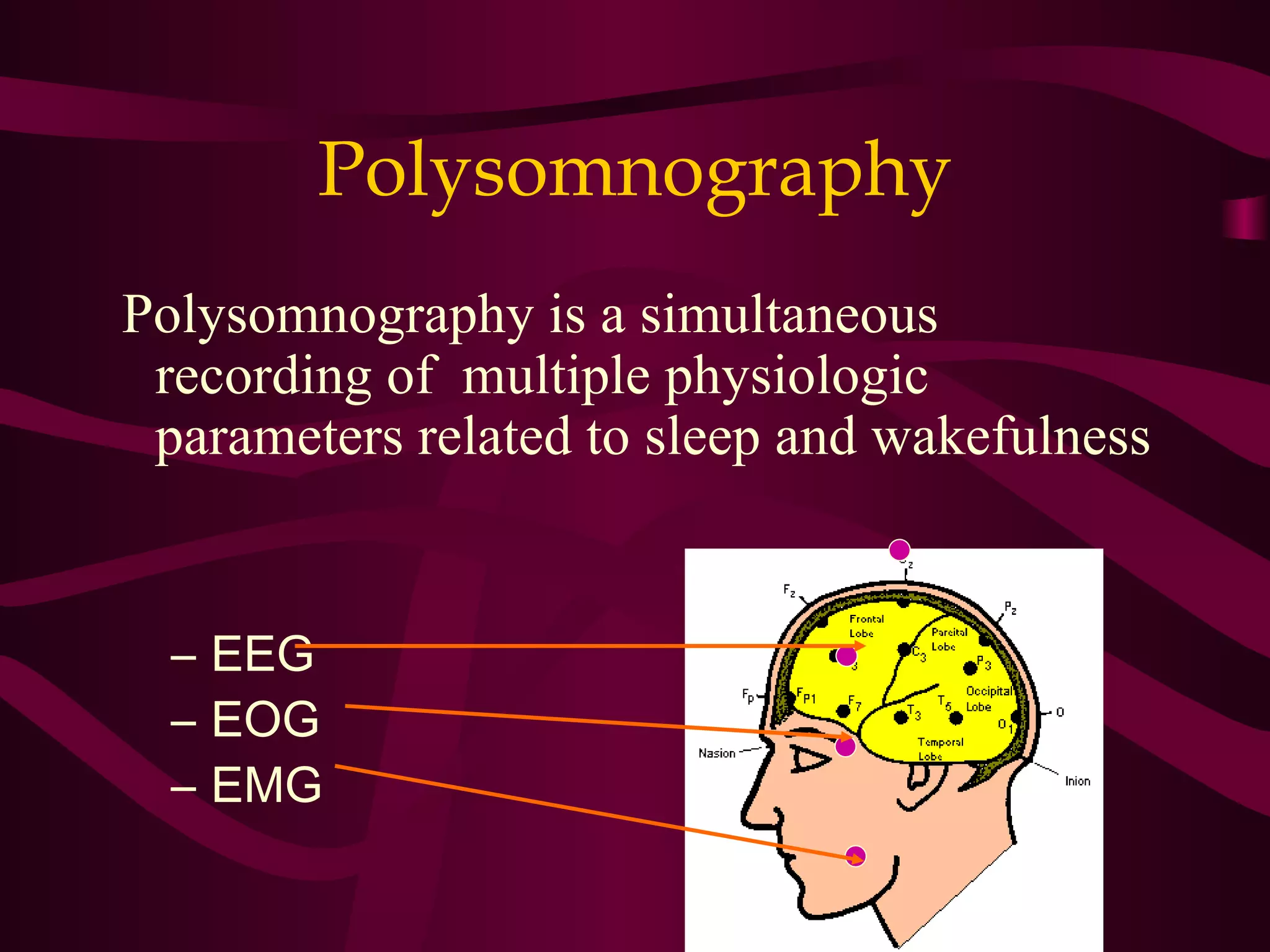


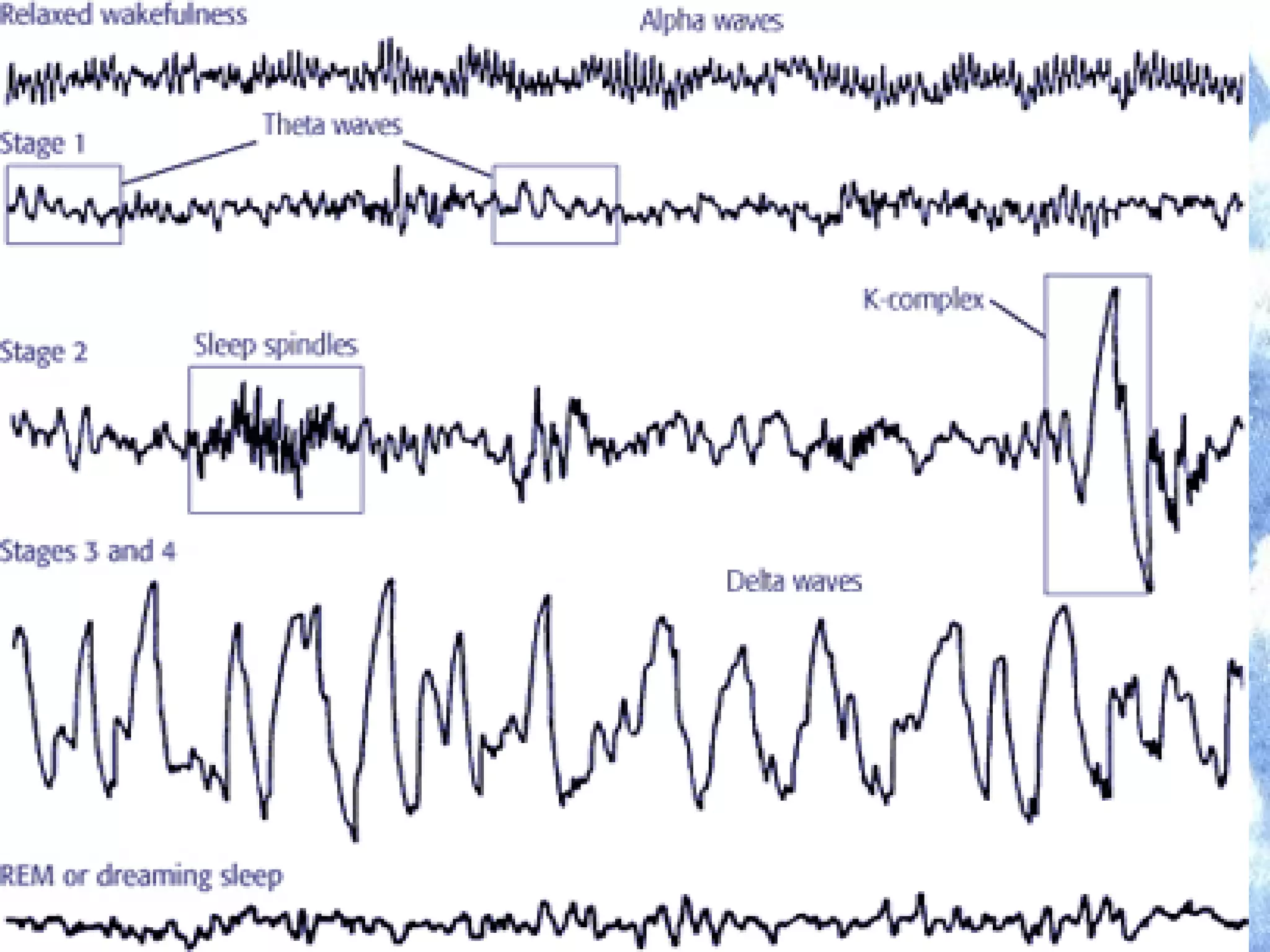

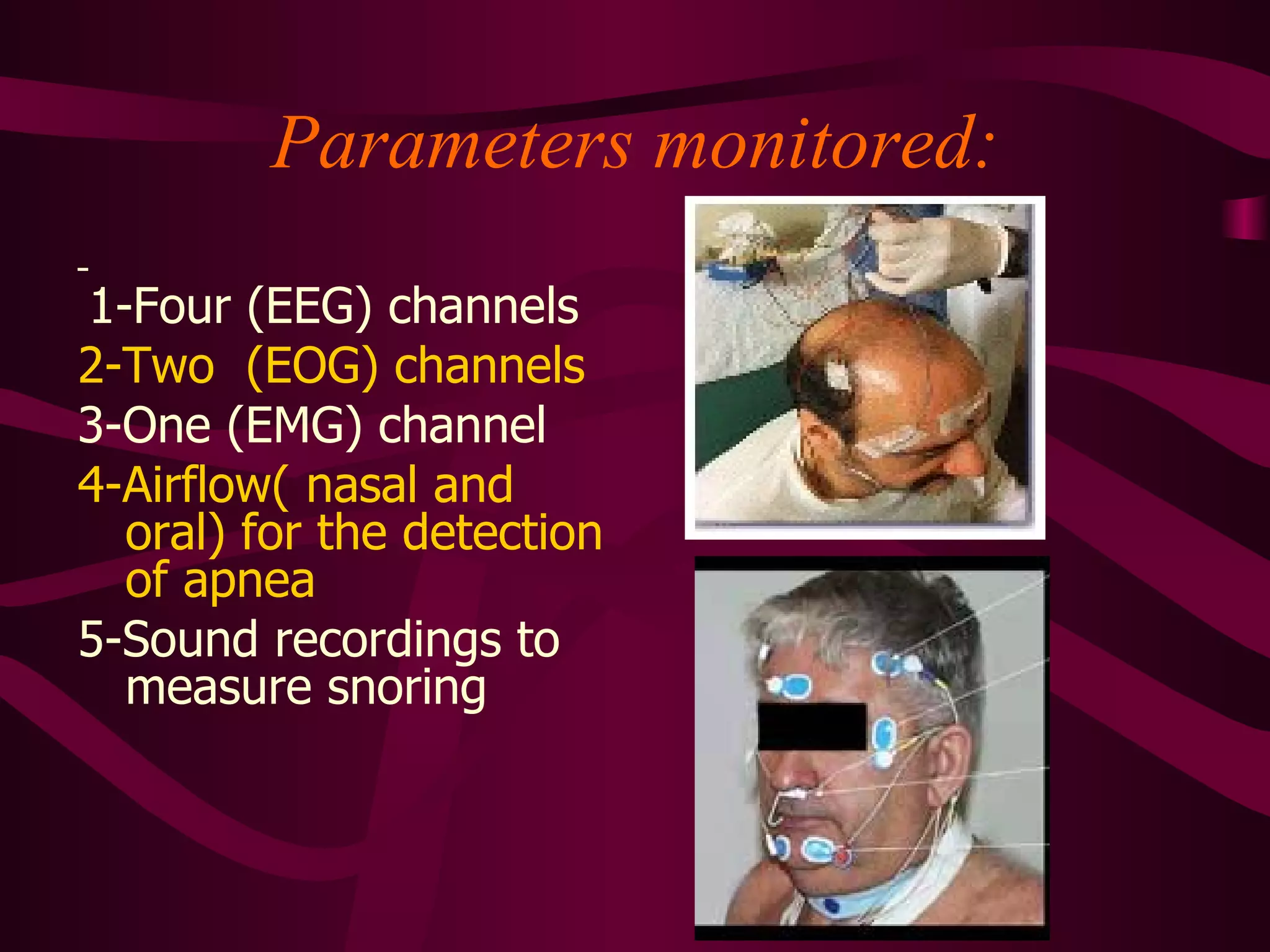
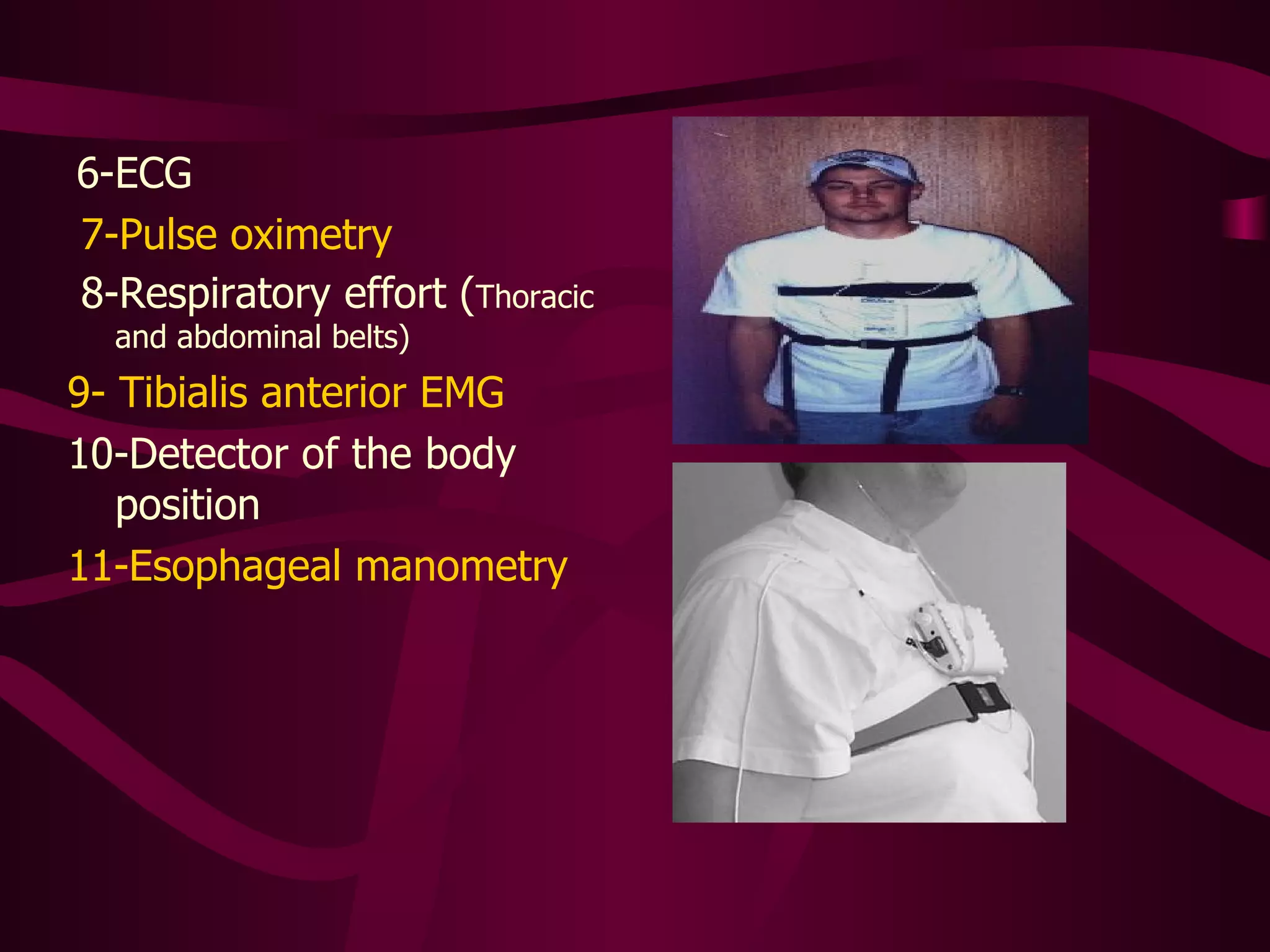
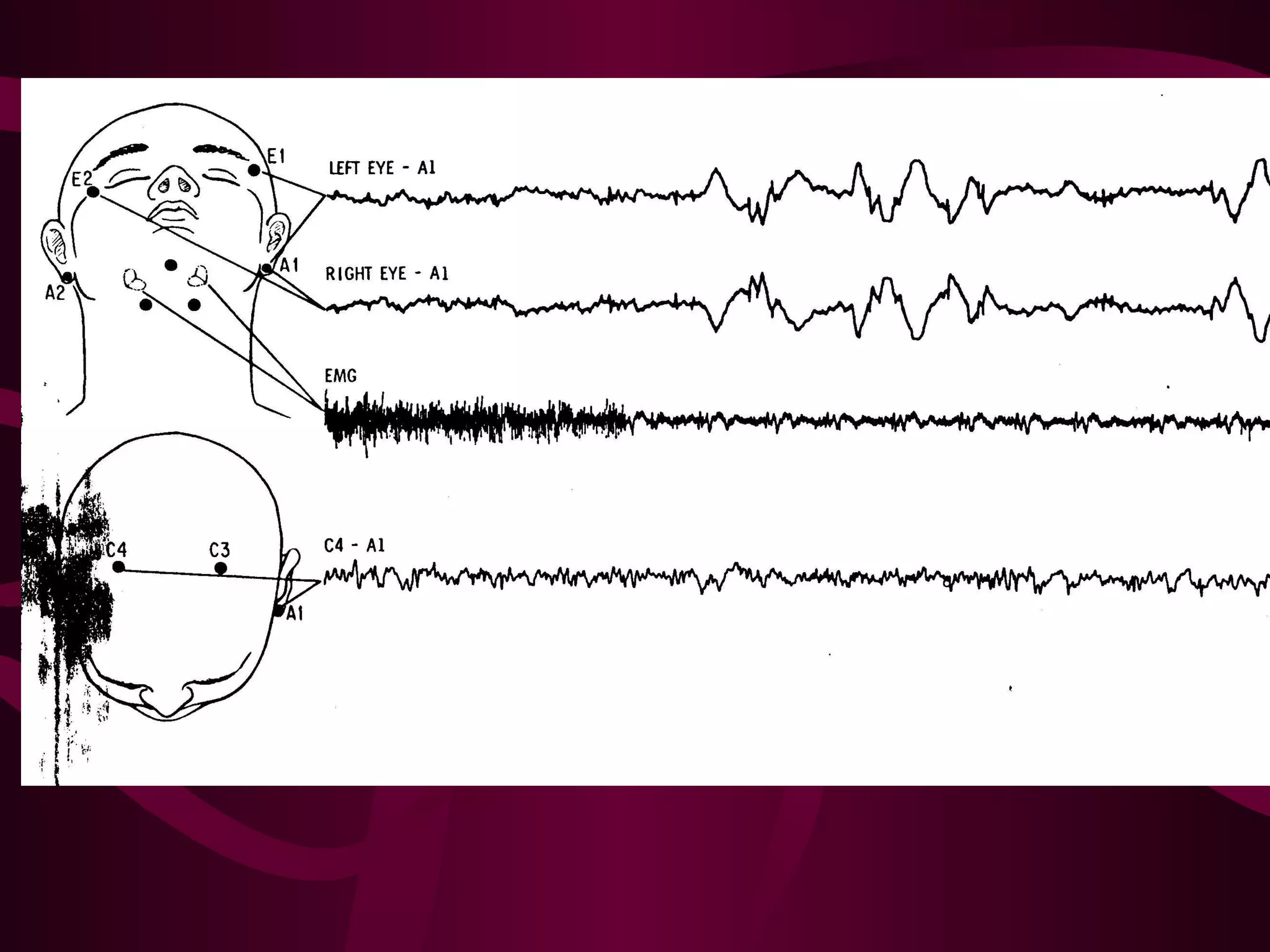
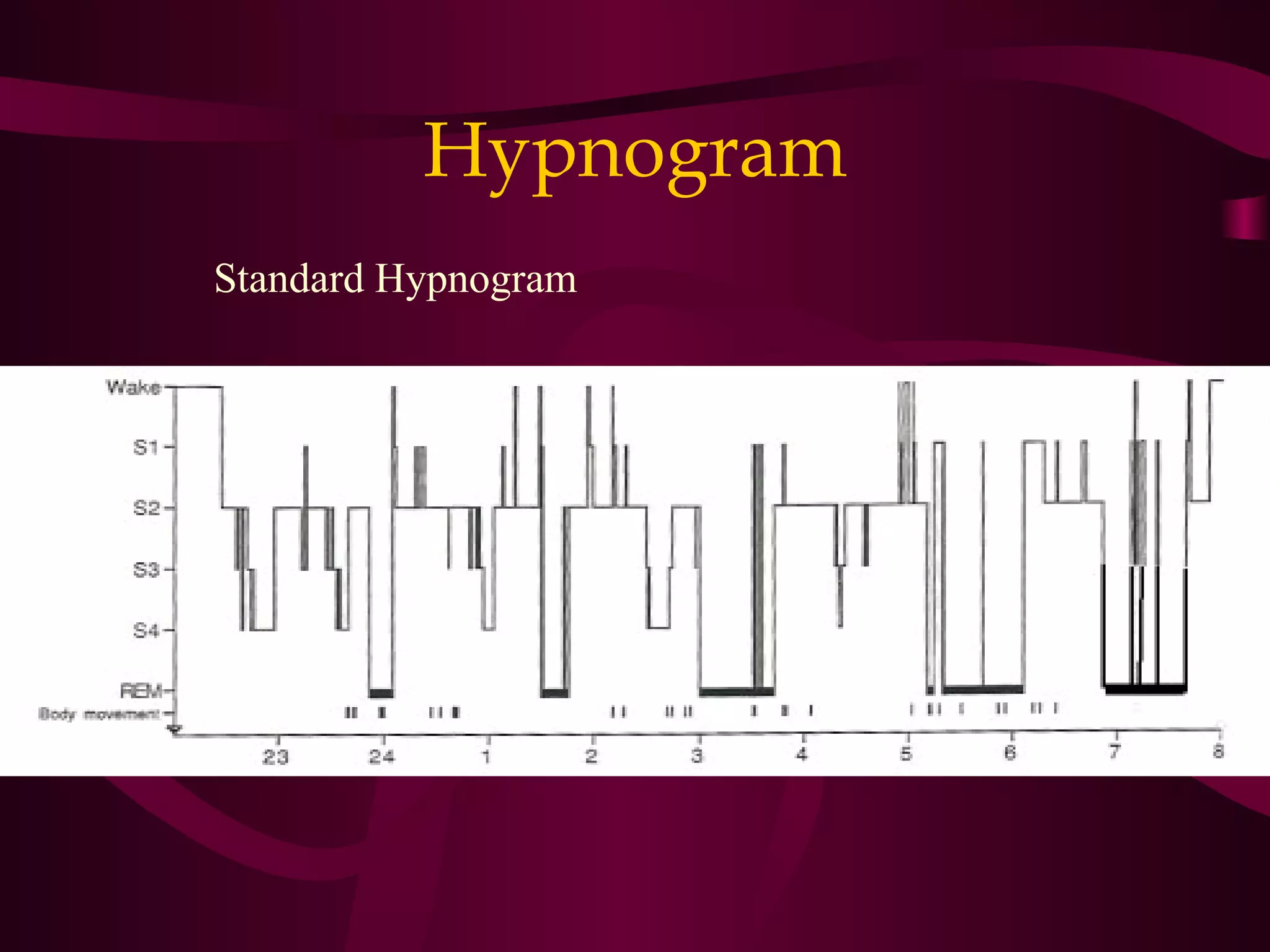
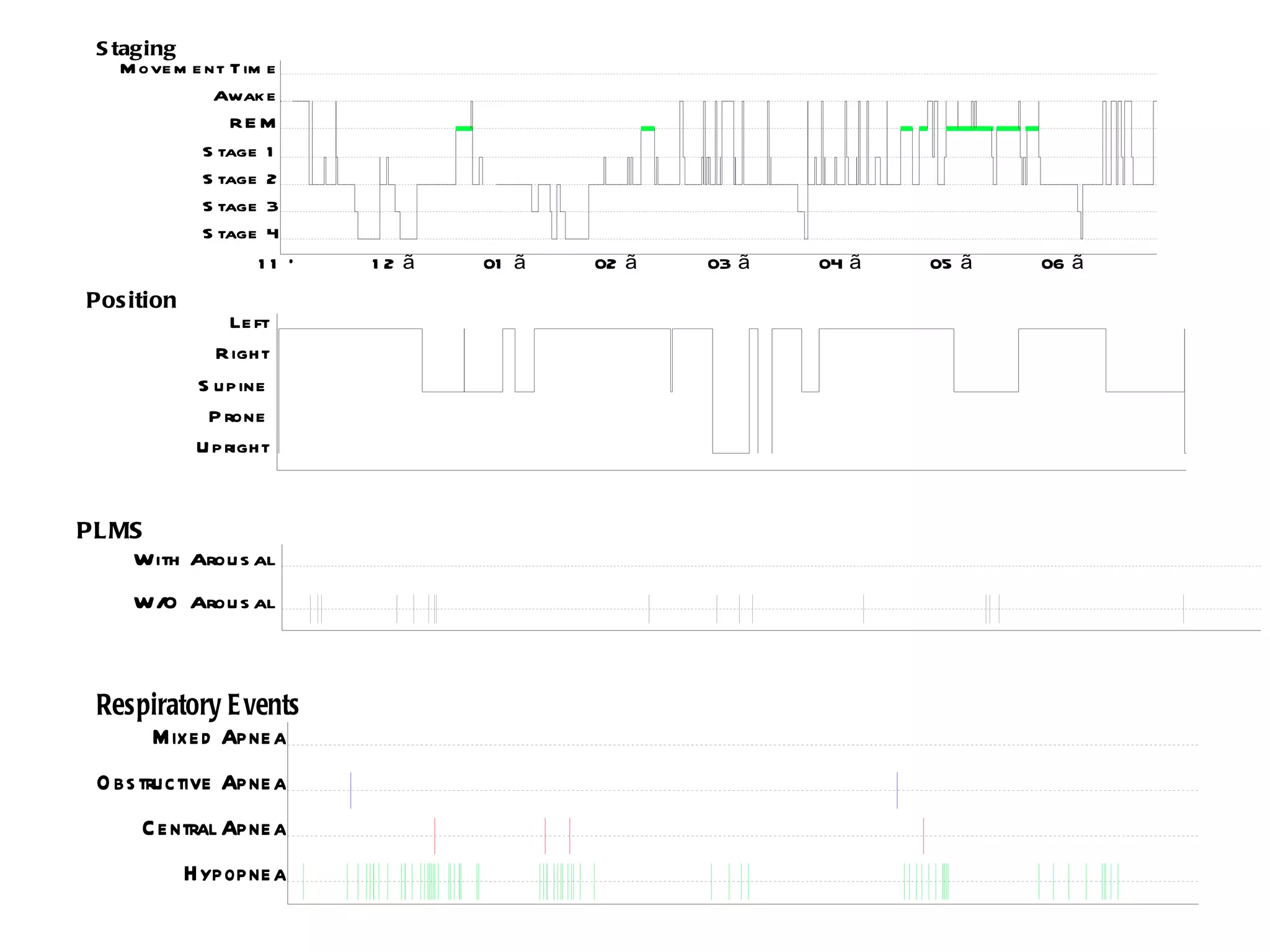
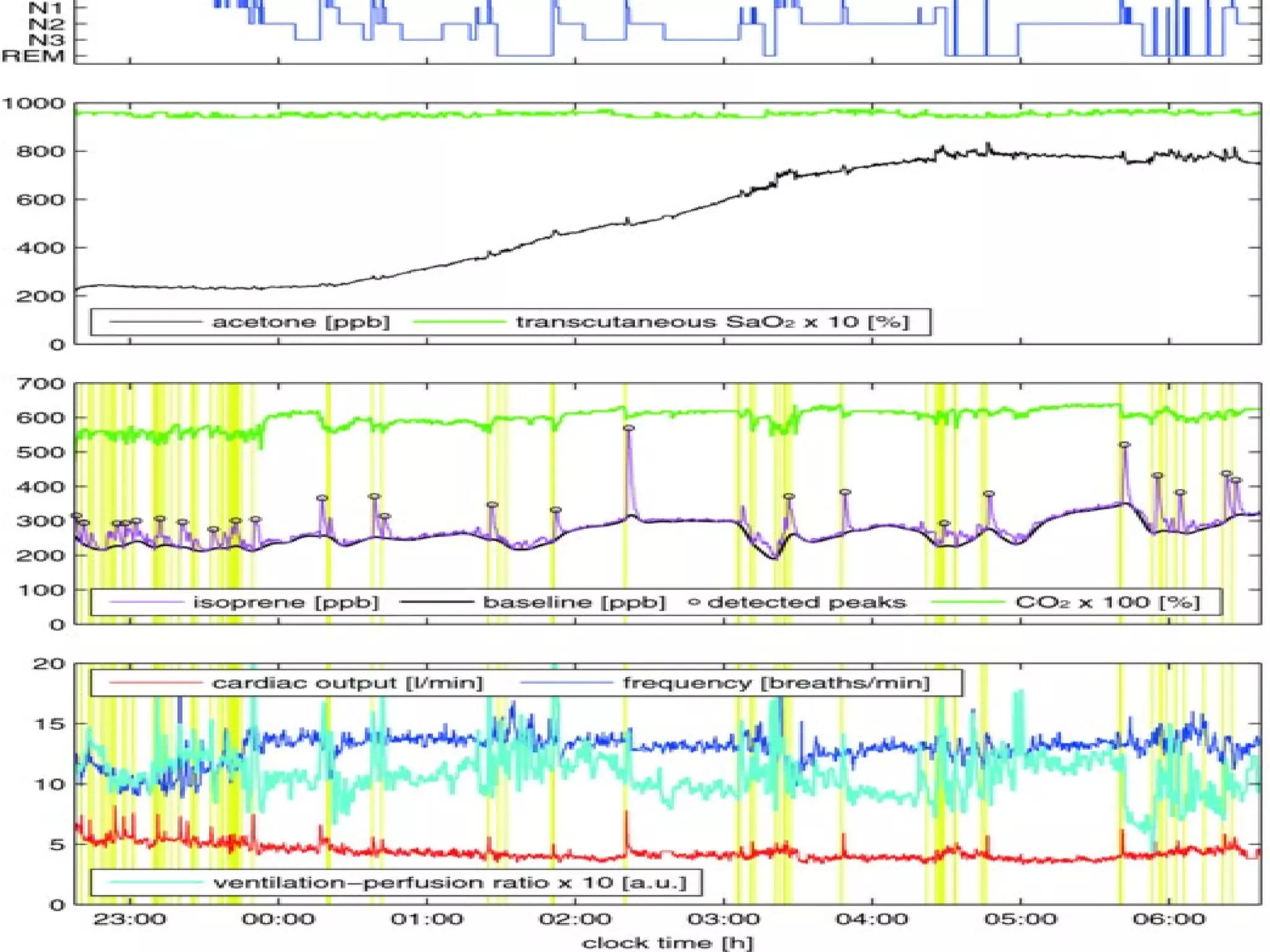
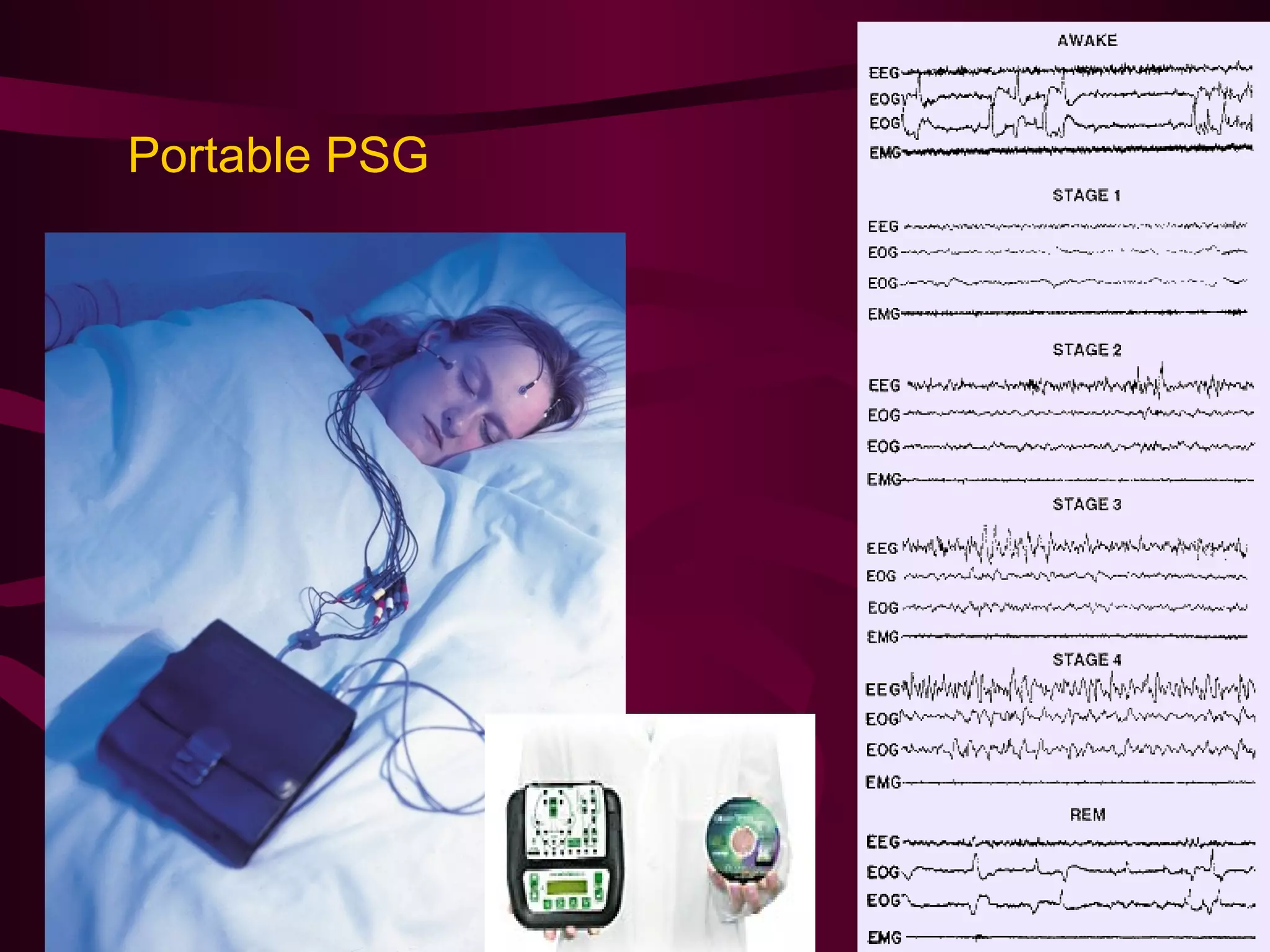
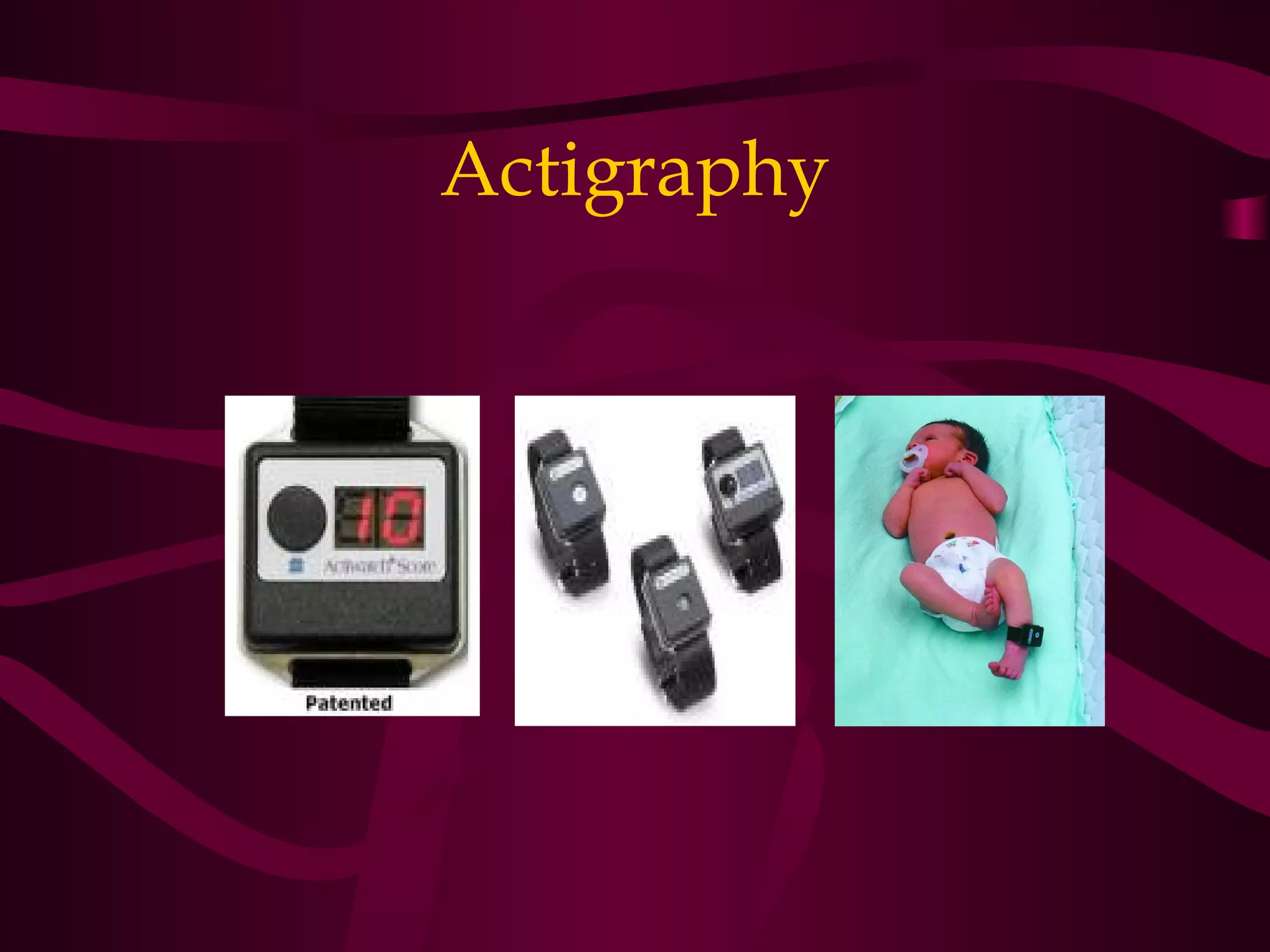



This document summarizes the history and milestones in the field of sleep medicine. It discusses investigations of sleep disorders including sleep history, medical history, examinations, laboratory tests, neurologic assessments, imaging studies, and sleep tests like polysomnography and multiple sleep latency tests. Key aspects of sleep physiology are reviewed such as sleep architecture, biological rhythms, and the neuroanatomy of sleep-wake regulation. Common sleep complaints and approaches to patient assessment are also outlined.











































![Sleep disorders [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/sleepdisordersautosaved-180531135608-thumbnail.jpg?width=640&height=640&fit=bounds)


















































