ASD EMBRYOLOGY, ECHOASSESSMENT AND DEVICE
CLOSURE
- DR. PRISCILLA
PG DNB CARDIOLOGY
2.
INTRODUCTION:
• ASD isthe most common congenital heart lesion in
adults and is often asymptomatic until adulthood.
• Diagnosis is important, as timely ASD repair improves
outcomes
3.
• ASDs resultfrom lack of sufficient tissue to completely
septate the atria and are classified according to their
location in the atrial septum.
• The location of the defect in relation to adjacent cardiac
structures defines the anomalies associated with the ASD
and impacts the natural history and requirements for
repair.
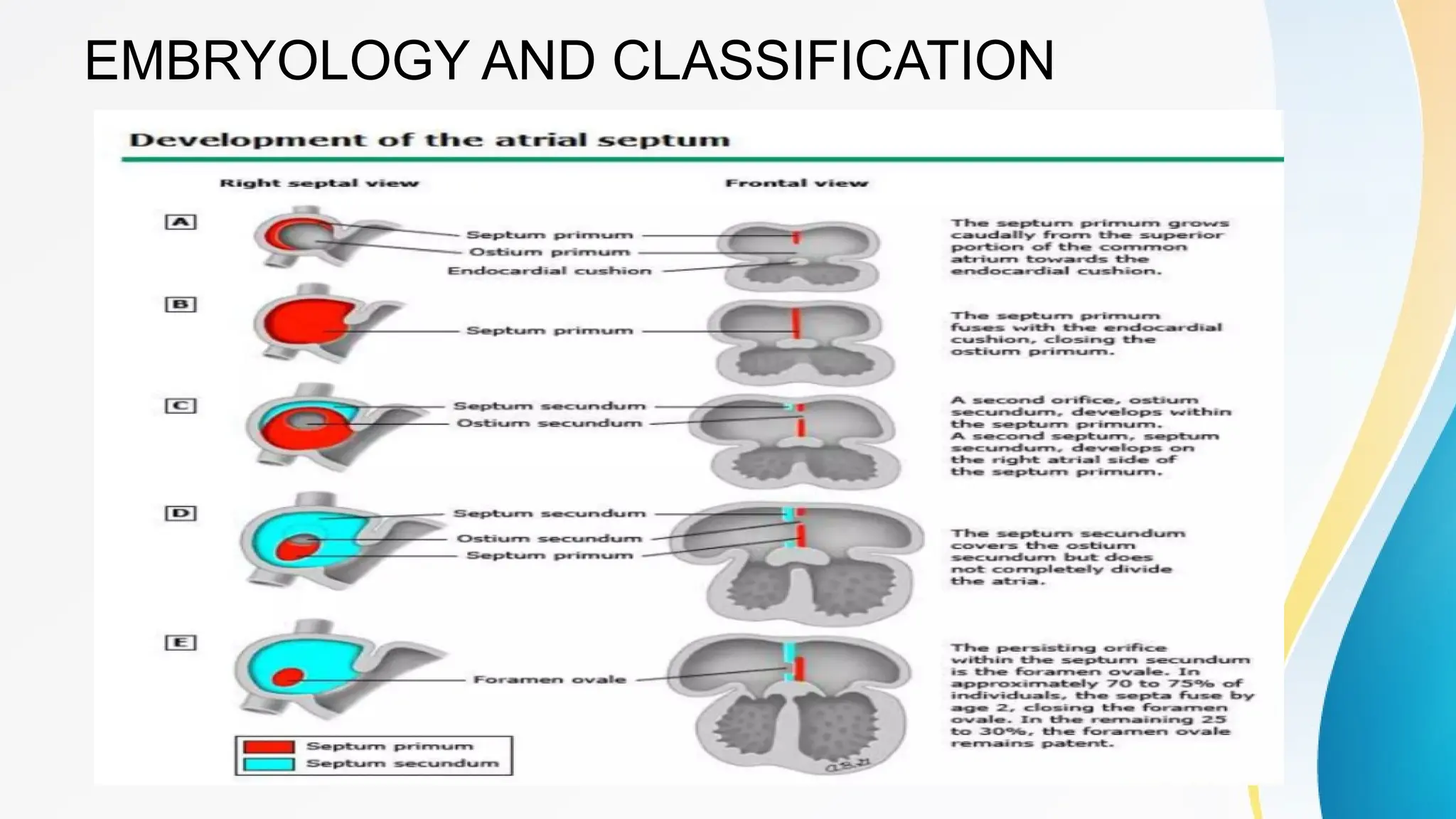
SEPTUM PRIMUM
• Thedevelopment of the normal atrial septum occurs
following the initial looping of the heart that is after 28
days of gestation.
• The initial step in septation, a ridge of tissue develops
from the superior aspect of the primary atrial component
of the heart tube.
• This ridge is the primary septum (septum primum), and its
the leading edge is covered by cushion-like mesenchymal
tissue that is continuous over the dorsal mesocardium.
11.
• As itgrows into the atrial cavity, it extends down towards
the endocardial cushions that are developing
concomitantly within the atrioventricular canal.
• Normal septal development also involves incorporation of
another mass of tissue derived from the dorsal
mesocardium.
12.
• This isknown as the vestibular spine (spina vestibuli),
and it also carries on its leading edge a mesenchymal
cap.
• As the primary septum approaches the atrioventricular
endocardial cushions, the various mesenchymal
structures fuse together. The mass derived from the
vestibular spine then muscularises, eventually forming the
prominent infero-anterior border of the oval foramen
13.
• After thefusion between the primary septum and the
endocardial cushions of the atrioventricular canal, the
upper part of the primary septum disintegrates to form the
‘ostium secundum’.
• Development of the ostium secundum occurs during the
fifth and sixth wks of embryologic life.
14.
• The remainingpart of the primary septum becomes the
flap valve of the oval fossa.
• This flap valve, along with the muscularised antero-
inferior rim, forms the true septum that separates the
cavities of the atrial chambers.
15.
• Flow throughthe foramen ovale is essential for fetal
circulation.
• The foramen ovale closes spontaneously within the first
two years of life in 70 percent of children.
• However, in a significant proportion (20 to 30 percent) of
the population, the septum does not fuse, leading to a
patent foramen ovale
16.
SEPTUM SECUNDUM
• Afterintegration of the pulmonary veins into the left atrium
the superior walls of the two atriums ‘infold’, creating the
“septum secundum” in the superior portion of the atriums.
• Septum secundum is also concave in shape, with the
concavity directed more posteriorly toward the opening of
the sinus venosus of the primitive heart.
• It has 2limbs- Superior and inferior.
• Inferior limb fuses with the lowest portion of the atrial
septum.
17.
• The flapvalve overlaps, but is not completely adherent to,
the rims of this superior atrial fold, also known as
Waterston's or Sonderggard's groove, providing a
passage during fetal life for blood to pass from the right to
the left atrium .
• The opening in the septum secundum is called the
foramen ovale.
19.
• Closure afterbirth –physiologically immediately
anatomically – 72 hours to 2 weeks .
• In about20% of cases, fusion of the septum primum and
septum secundum is incomplete,and a narrow oblique
cleft remains between the two atria.
• This condition is called probe patency of the oval
foramen; it does not allow intracardiac shunting of blood.
20.
SECUNDUM ASD:
• SECUNDUMASD accounts for 70 to 75 percent of all
ASDs.
• Secundum ASD is a defect in the septum primum
resulting from poor growth of the secundum septum or
excessive absorption of the septum
• Although most secundum ASDs are isolated defects,
familial forms exist, some of which are associated with
other congenital cardiac and extracardiac abnormalities.
21.
• Other geneslinked to familial isolated secundum ASD
include GATA 4,MYH6, NKX2-5.
• These syndromes typically present in childhood or
adolescence
• The genetic disorder associated with secundum ASD is
the HOLT ORAM SYNDROME (also known as heart-hand
syndrome) which is caused by various mutations, most
commonly mutations in the TBX5 gene
22.
• Secundum ASDsare occasionally associated with partial
anomalous pulmonary venous connection and/or
pulmonary stenosis.
• The rare combination of an ASD with rheumatic mitral
stenosis is known as Lutembacher syndrome.
24.
Primum ASD
• PrimumASD accounts for 15 to 20 percent of ASDs.
• A primum ASD is a defect in the septum secundum
caused by failure of the primum septum to fuse with the
endocardial cushions at the base of the interatrial septum.
• This results from maldevelopment/malalignment of the
ventricular septum due to malformation of the endocardial
cushions rather than a decrease in atrial septal tissue.
25.
• Primum ASDsare nearly always associated with
anomalies of the atrioventricular (AV) valves, particularly a
cleft in the anterior mitral valve leaflet, with or without a
contiguous defect in the inlet ventricular septum.
• When the combination of the primum ASD, cleft mitral
valve, and an inlet ventricular septal defect are seen, this
is called a partial AV septal defect (AVSD).
26.
• The mostsevere form of AVSD (or endocardial cushion
defect) is the complete AV septal (or canal) defect, in
which a primum ASD and inlet ventricular septal defect
are present along with a common AV valve
• The most severe form of AVSD (or endocardial cushion
defect) is the complete AV septal (or canal) defect, in
which a primum ASD and inlet ventricular septal defect
are present along with a common AV valve
29.
Sinus venosus defect
•Sinus venosus defects account for 5 to 10 percent of
ASDs and are located in the venoatrial portion of the atrial
septum.
• Sinus venosus defects represent an abnormality in the
insertion of the superior or inferior vena cava, which
overrides the interatrial septum; the interatrial
communication is then formed within the mouth of the
overriding vein and is outside the area of the fossa
ovalis .
30.
• Thus, sinusvenosus defects are technically not ASDs
since the defect is within the sinus venosus septum.
• An anomalous connection involving one or more
pulmonary veins is present in most patients with sinus
venosus ASD
• Sinus venosus defects are of two types:
– SUPERIOR SINUS VENOSUS ASD
– INFERIOR SINUS VENOSUS ASD
31.
SUPERIOR SINUS VENOSUSASD:
• Superior sinus venosus defects are located immediately
below the orifice of the superior vena cava.
• The right upper lobe and middle lobe pulmonary veins
often connect to the junction of the superior vena cava
and right atrium or on the superior vena cava, resulting in
a partial anomalous pulmonary venous connection
32.
INFERIOR SINUS VENOSUSASD:
• Inferior sinus venosus defects, also known as inferior
vena caval defects, are much less common.
• They are located immediately above the orifice of the
inferior vena cava.
• These defects are also often associated with partial
anomalous connection of the right pulmonary veins to the
junction of the right atrium and inferior vena cava.
33.
Unroofed coronary sinus:
•Unroofed coronary sinus (also known as coronary sinus
defect) is caused by absence of part or all of the common
wall between the coronary sinus and the left atrium.
• This defect accounts for less than 1 percent of ASDs and
is commonly associated with a persistent left superior
vena cava.