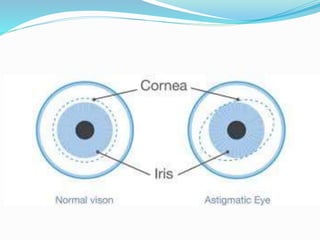
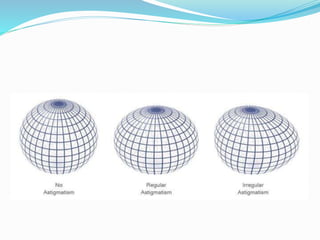
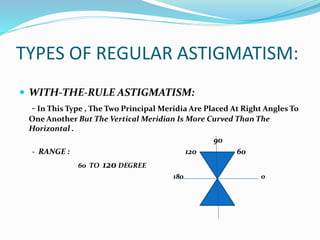
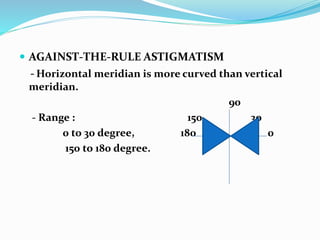
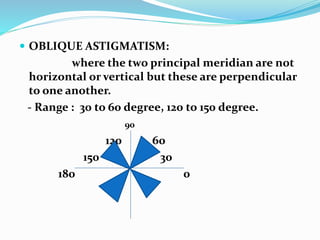
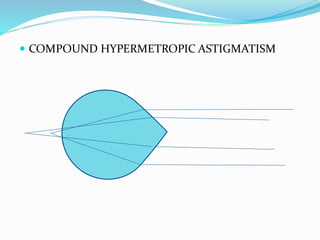
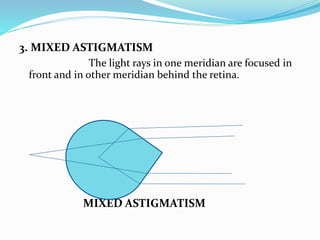
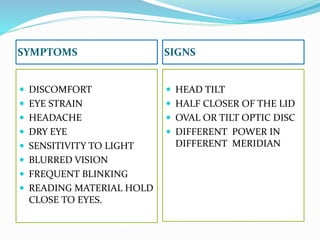
Astigmatism occurs when parallel rays of light focus at multiple points rather than a single point due to differences in curvature along the eye's meridians. There are two types: regular astigmatism where curvature changes uniformly between meridians, and irregular astigmatism with non-uniform changes. Regular astigmatism is further classified as with-the-rule, against-the-rule, or oblique based on meridian angles. Symptoms include blurred vision, eye strain, and headaches. Treatment options include optical correction with glasses or contacts, or refractive surgery.