



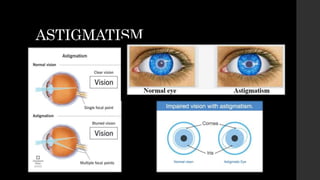













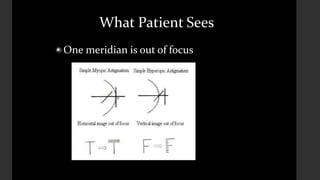




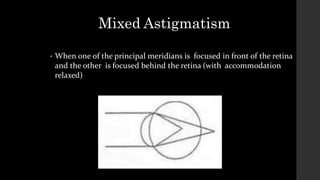













Astigmatism is a condition where light rays are not focused to a single point on the retina due to irregular curvature of the cornea or lens. It can be classified based on etiology, orientation of refractive meridians, and location of focal points relative to the retina. Symptoms include distorted vision and headaches. It is diagnosed using visual acuity and refraction tests. Treatment options include spectacles, contact lenses, and refractive surgery to correct the refractive error.























































































