Downloaded 35 times




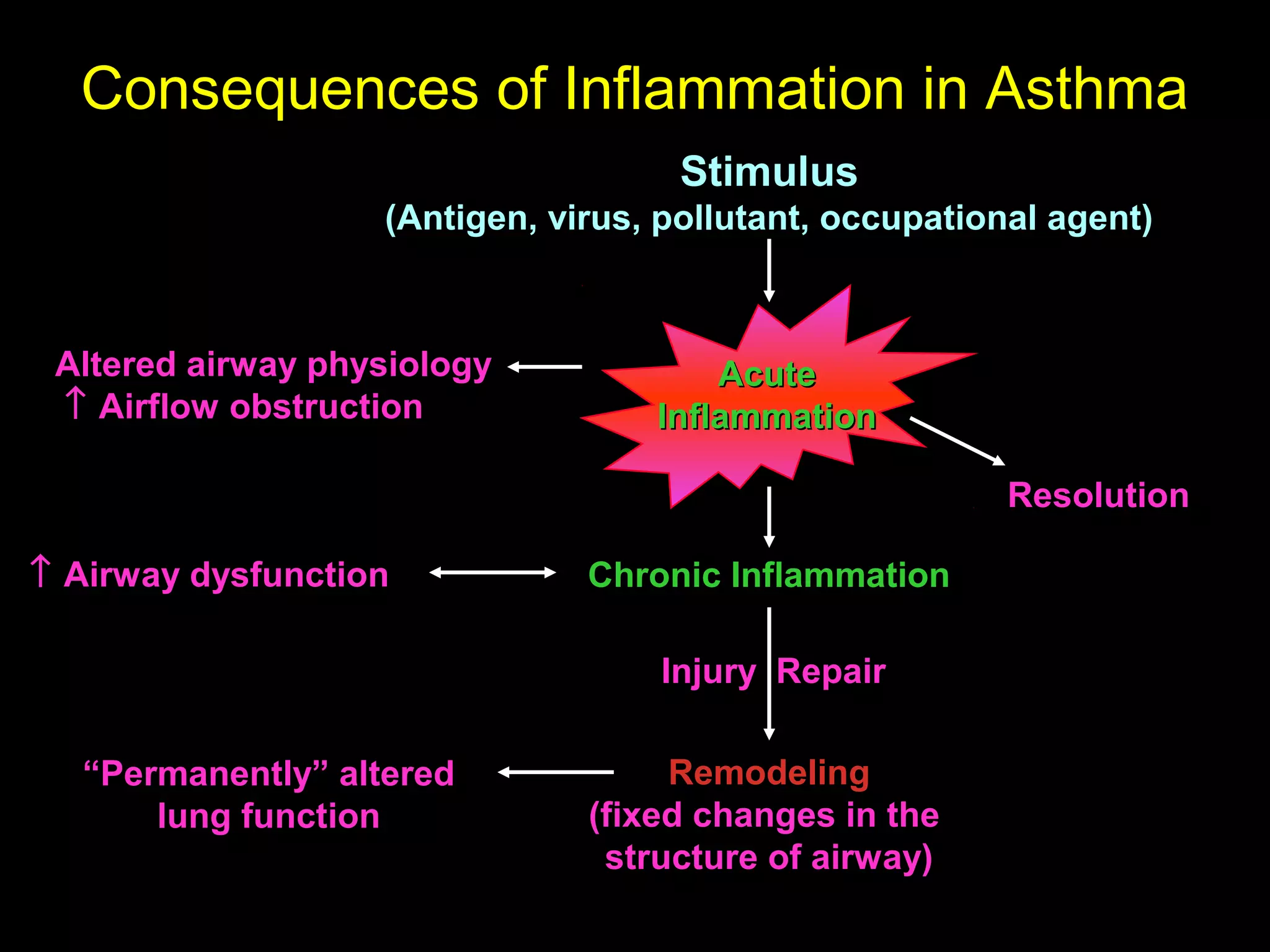
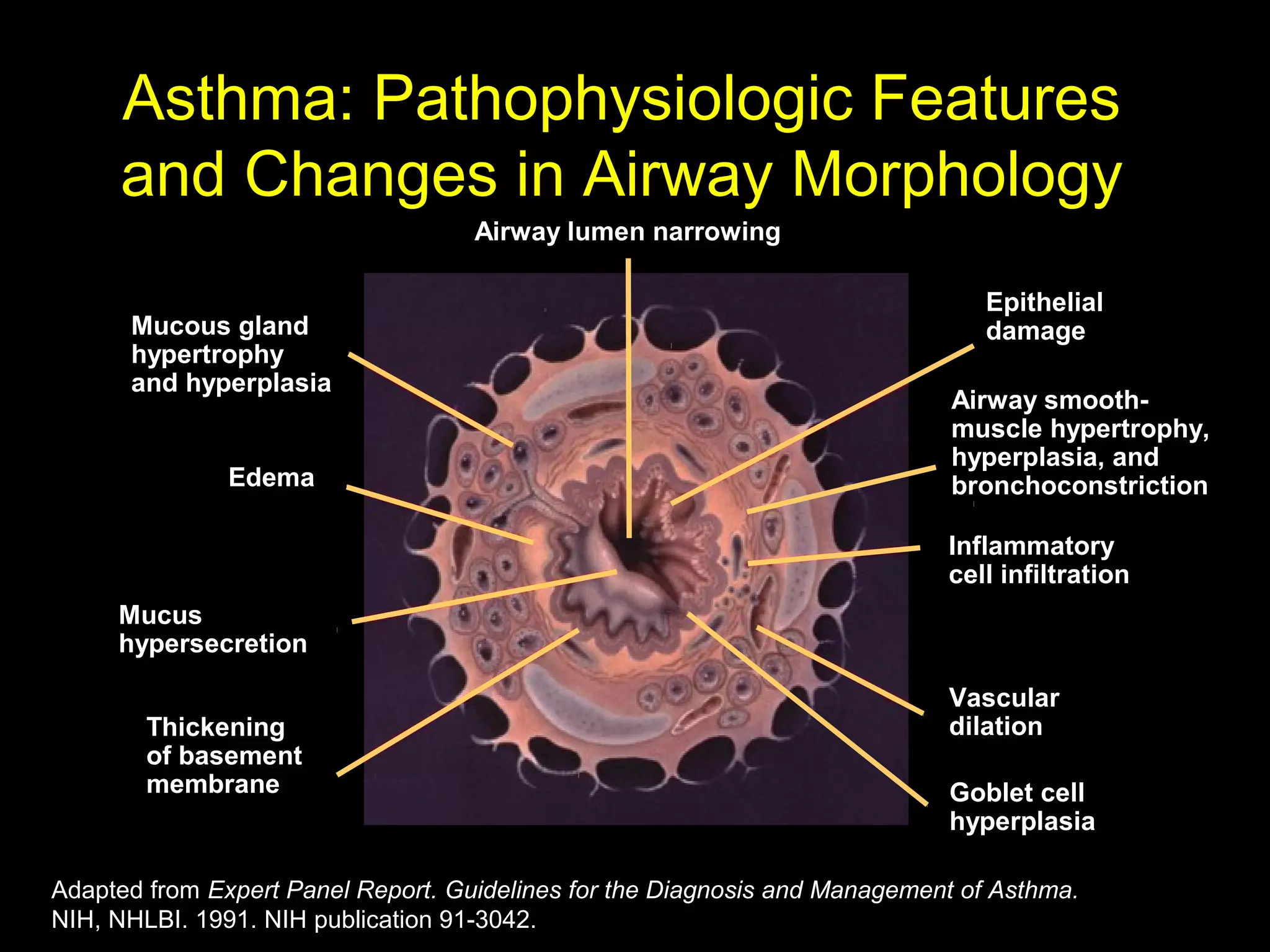

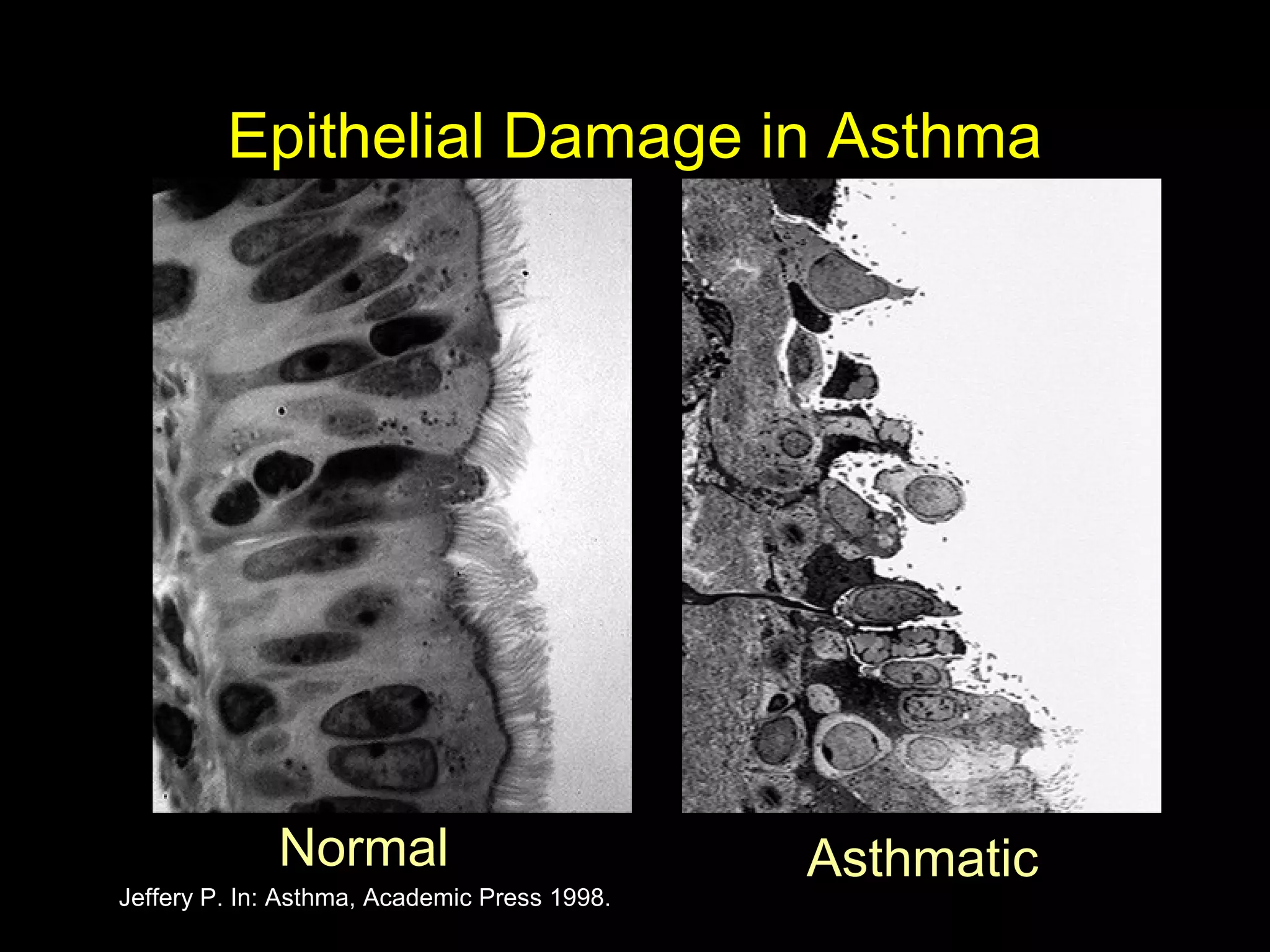
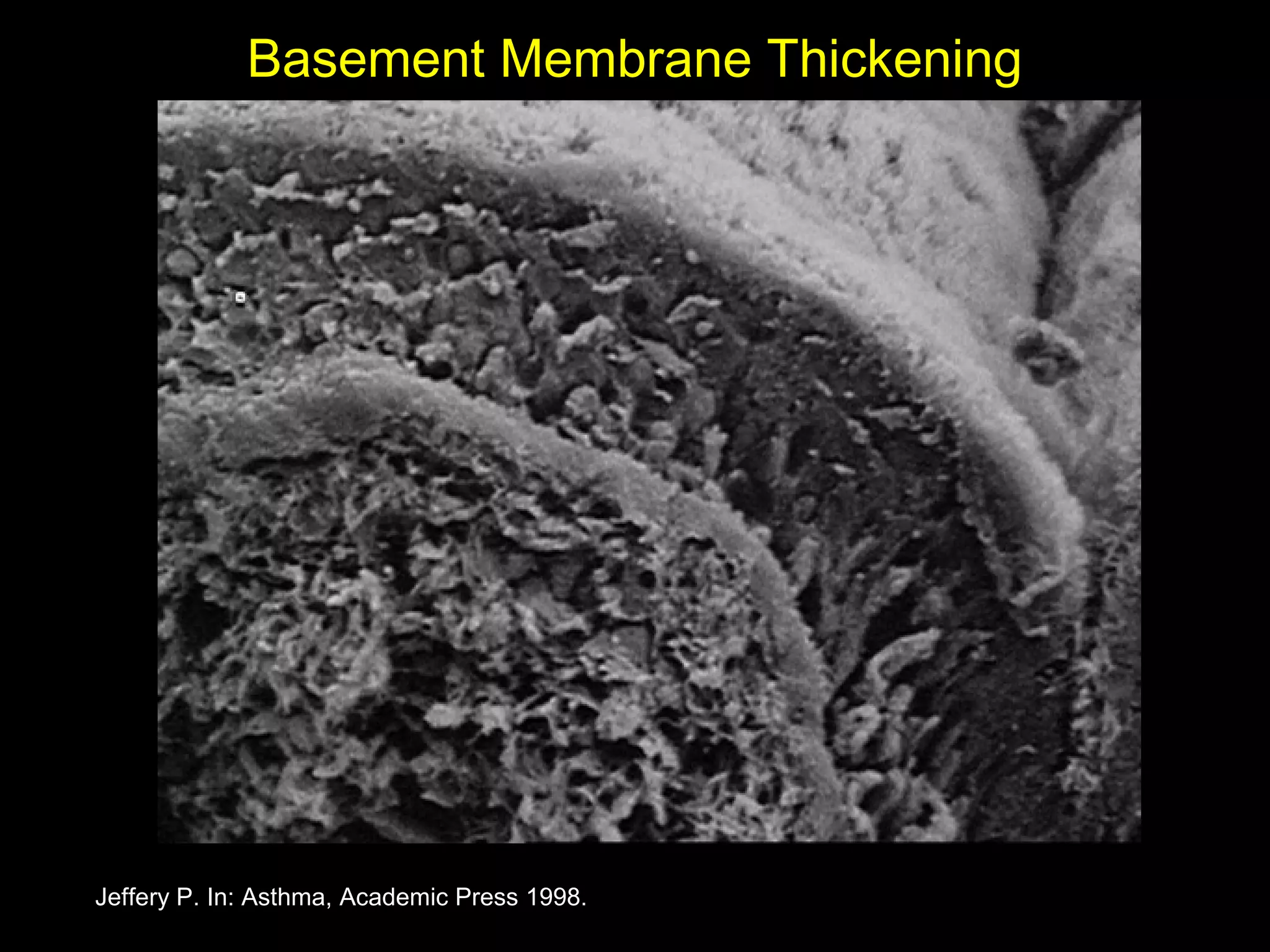











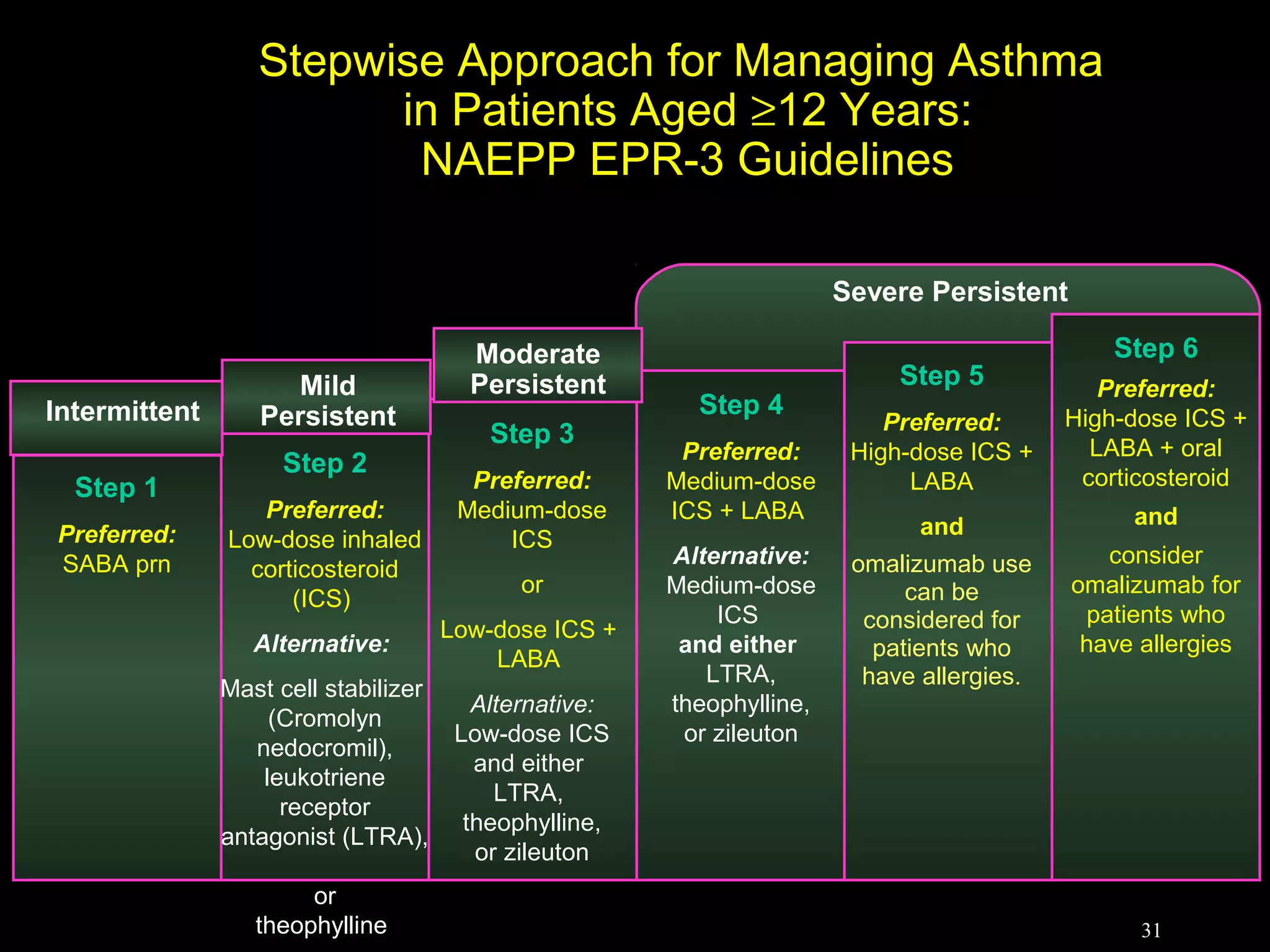





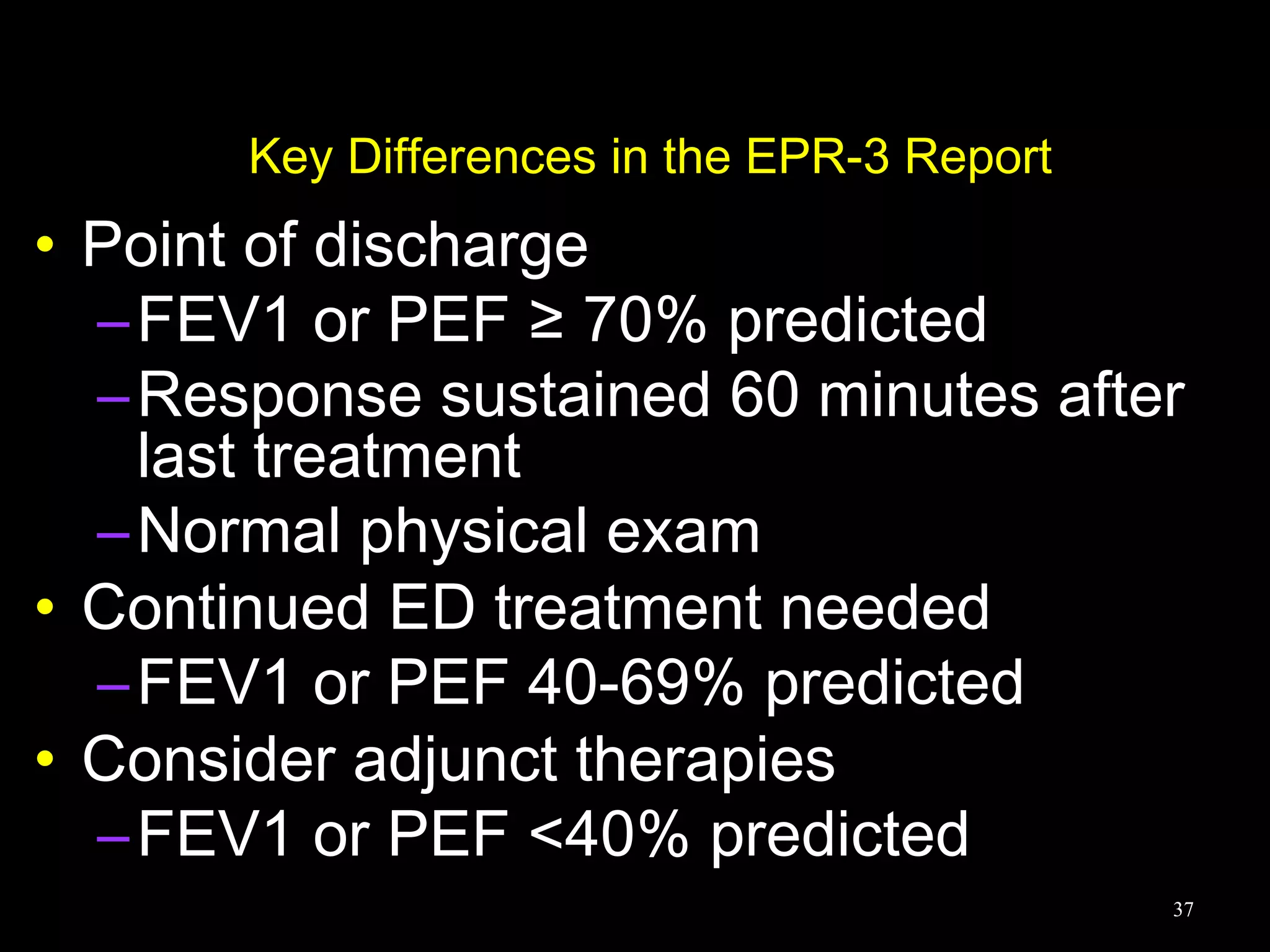

- Asthma is a chronic lung disease characterized by airway inflammation and narrowing of the airways. It causes symptoms like wheezing, coughing, and shortness of breath. - It is diagnosed based on a patient's medical history and symptoms, and confirmed via spirometry testing which shows improved lung function after use of a bronchodilator. - Treatment involves controlling triggers, medications like inhaled corticosteroids to reduce inflammation, and managing exacerbations which involve increasing medications under a treatment plan.












































![Microsoft PowerPoint - Asthma 4th year Lecture (1) [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/microsoftpowerpoint-asthma4thyearlecture1compatibilitymode-220716165932-01cf3f8c-thumbnail.jpg?width=640&height=640&fit=bounds)

![Microsoft+PowerPoint+-+Asthma+4th+year+Lecture+(1)+[Compatibility+Mode].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/microsoftpowerpoint-asthma4thyearlecture1compatibilitymode-230704125445-487a63ed-thumbnail.jpg?width=640&height=640&fit=bounds)































