CHILDHOOD ASTHMA
PROF. DR.SAMIYA NAEEMULLAH
Diplomate American Board of Pediatrics
F.A.A.P. FCPS
Head of Department of Pediatrics
Rawalpindi Medical College
2.
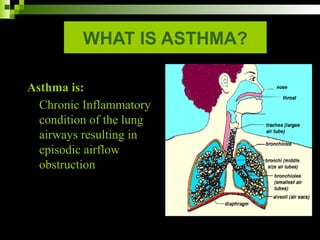
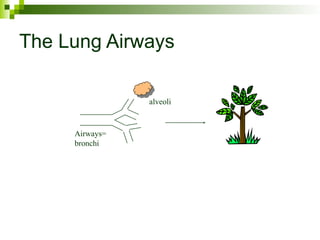
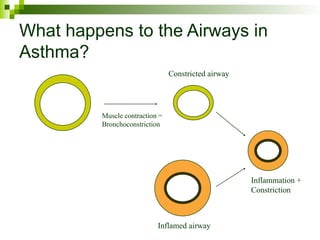
WHAT IS ASTHMA?
Asthmais:
Chronic Inflammatory
condition of the lung
airways resulting in
episodic airflow
obstruction
3.
PRESENTATION
Characterized byrecurrent breathing problems
Manifests as
Breathlessness
Wheezing
Chest tightness, and coughing
Asthma symptoms varyfrom:
Hour to hour
Day to day
Week to week
Over months
Worse at night and in the early hours of the morning.
The severity of asthma also varies from individual to
individual.
6.
CHILD FREE OFSYMPTOMS BETWEEN
ATTACKS
& NORMAL PHYSICAL EXAMINATION OF
CHEST
7.
Who are affectedby Asthma
All ethnic groups.
Socioeconomic levels.
Ages
Asthma often develops during childhood.
50% under 1 year affected.
80-90% under 5 years
8.
GENETICS
Asthma:
One parent affected:
25%chance
Both parents affected:
50% chance
10% if no F/H
Incidence in Twins:
Monozygotic 74%
Diazygotic 35%
All other allergies:
One parent affected:
50% chance
Both parents affected:
66% chance
9.
Global burden ofAsthma report
On world Asthma day May 04, 2004 the
Global Initiative for Asthma 300 million
world wide.
1998 statistics by NCHS (National Centre for
Health Statistics)
8.65 million children (12.1%).
3.8 million children have experienced an
asthma episode in US in preceding 12
months.
10.
Under Diagnosed& Under Treated Condition worldwide.
Increasing incidence.
Besides improvements in medication.
In US 1982-1994 72%
ISAAC (1.6 – 36.8%)
DIAGNOSIS
History + physicalexamination
CBC – normal
Eosinophilia
Immunoglobulins
Sweat test
Mantoux test
Radiographs
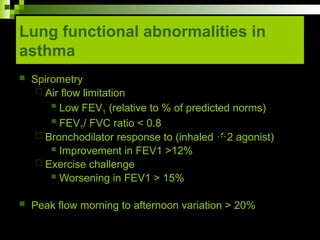
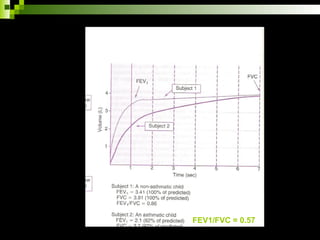
Lung function test
Blood gases
Allergy skin testing
Rast
Asthmatics are classifiedas:
Intermittent -
Asthmatics who have symptoms that occur
with a cold from time to time.
They often grow out of the disease.
Persistent -
Asthmatics having symptoms at least twice a week
during the day and twice a month during the night.
These asthmatics are further classified as mild,
moderate, or severe.
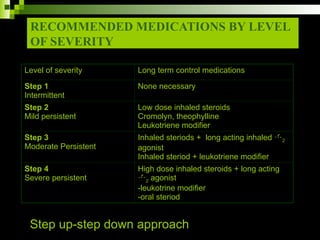
35.
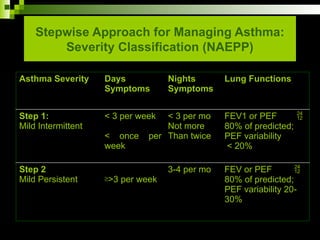
Stepwise Approach forManaging Asthma:
Severity Classification (NAEPP)
Asthma Severity Days
Symptoms
Nights
Symptoms
Lung Functions
Step 1:
Mild Intermittent
< 3 per week
< once per
week
< 3 per mo
Not more
Than twice
FEV1 or PEF
80% of predicted;
PEF variability
< 20%
Step 2
Mild Persistent ³>3 per week
3-4 per mo FEV or PEF
80% of predicted;
PEF variability 20-
30%
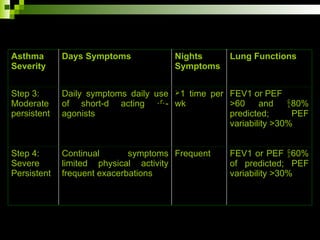
36.
Asthma
Severity
Days Symptoms Nights
Symptoms
LungFunctions
Step 3:
Moderate
persistent
Daily symptoms daily use
of short-d acting -
agonists
1 time per
wk
FEV1 or PEF
>60 and 80%
predicted; PEF
variability >30%
Step 4:
Severe
Persistent
Continual symptoms
limited physical activity
frequent exacerbations
Frequent FEV1 or PEF 60%
of predicted; PEF
variability >30%
37.
Management and Prevention
Develop patient/doctor partnership
Identify and reduce exposure to risk factors
Assess, treat and monitor asthma
Manage asthma exacerbations
Special considerations
38.
Aim of partnership
To give people with asthma the ability to control their
own condition and guidance from healthcare
professionals
To discuss goals of treatment
Develop written self management Action Plan
Identify and reduceexposure to risk
factors
Prevent allergic sensitization prenatally
Inhibit exposure to tobacco smoke prenatally and
postnatally
Breast feeding
Prevention from outdoor and indoor allergens
Any other triggers
Drugs ( aspirin and beta blockers )
Influenza vaccination
Obesity
Emotional stress
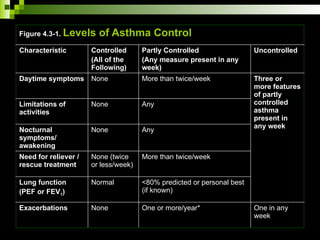
Figure 4.3-1. Levelsof Asthma Control
Characteristic Controlled
(All of the
Following)
Partly Controlled
(Any measure present in any
week)
Uncontrolled
Daytime symptoms None More than twice/week Three or
more features
of partly
controlled
asthma
present in
any week
Limitations of
activities
None Any
Nocturnal
symptoms/
awakening
None Any
Need for reliever /
rescue treatment
None (twice
or less/week)
More than twice/week
Lung function
(PEF or FEV1)
Normal <80% predicted or personal best
(if known)
Exacerbations None One or more/year* One in any
week
44.
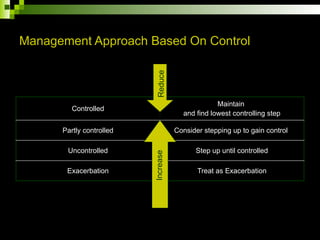
Management Approach BasedOn Control
Controlled
Maintain
and find lowest controlling step
Partly controlled Consider stepping up to gain control
Uncontrolled Step up until controlled
Exacerbation Treat as Exacerbation
Increase
Reduce
45.
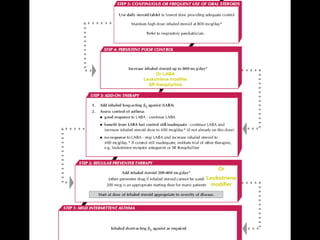
Asthma pharmacotherapy
Long-termcontrol versus quick-relief medications
Classification of asthma severity for anti-inflammatory
pharmacotherapy
Step-up, step-down approach
Asthma exacerbation management
46.
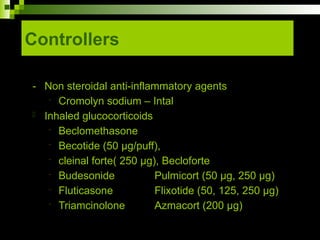
Asthma medications
Quickrelief medications
“Relievers” “Rescue”
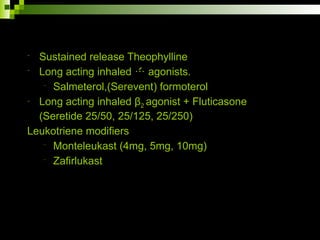
Long term control medications
“controllers”
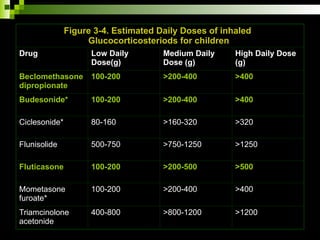
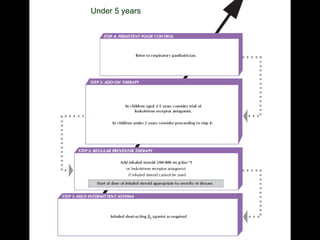
Figure 3-4. EstimatedDaily Doses of inhaled
Glucocorticosteriods for children
Drug Low Daily
Dose(g)
Medium Daily
Dose (g)
High Daily Dose
(g)
Beclomethasone
dipropionate
100-200 >200-400 >400
Budesonide* 100-200 >200-400 >400
Ciclesonide* 80-160 >160-320 >320
Flunisolide 500-750 >750-1250 >1250
Fluticasone 100-200 >200-500 >500
Mometasone
furoate*
100-200 >200-400 >400
Triamcinolone
acetonide
400-800 >800-1200 >1200
52.
THE “3 STRIKES”RULE
The child should receive controller therapy based on
NAEPP Guidelines
If an asthmatic child requires
Quick-relief medication more than 3 times per week
Awakens at night due to asthma more than 3 times per
month
Requires refill for a quick-relief inhaler more than 3 times
per year
Maintain normalactivity
Regular school or daycare attendance
Full participation in physical exercise, athletics, and
other recreational activities
Prevent sleep disturbance
Prevent chronic asthma symptoms
Keep asthma exacerbations from becoming severe
Maintain normal lung function
Experience little to no adverse effects of treatment
57.
Four Components ofOptimal
Asthma Management
Regular assessment and monitoring
Asthma check-ups
Every 2-4 wk until good control is achieved
2-4 per year to maintain good control
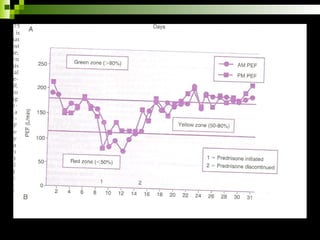
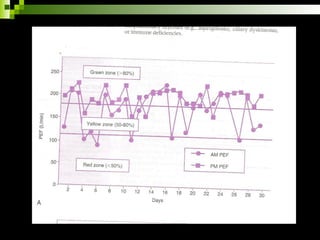
Lung function monitoring
Control on medication at any step for three months step
up or step down
Review and followup
58.
PROGNOSIS
Ultimate remissiondepends on growth and cross-
sectional diameter of the airways
50% of all asthmatic become symptom free with 10-20
years
Onset between two years and puberty
Remission rate 50%
Children with severe asthma
Frequent hospitalizations and steroid dependent
disease
95% become adult asthmatics
Ludwig vanBeethoven, composer
Leonard Bernstein, conductor
Bob Hope, entertainer
Samuel Johnson, 18th century poet, critic, and writer
John F. Kennedy, 35th president of the United States
Peter the Great, 18th century Russian czar
William Tecumseh Sherman, Civil War General
Elizabeth Taylor, actress
Charles Dickens, novelist
Jim “Catfish” Hunter, baseball Hall of Famer
Greg Louganis, Olympic diver
Did you know these famous people also suffered from,
or currently suffer from asthma?
61.
Threshold concentrations ofallergens
10 ug/g dust of group I mite allergen
8 ug/g dust of Fel d I,the major cat allergen
10 ug/g dust of Can f I,the major dog allergen
8 ug/g dust of cockroach allergen
62.
Asthma Quiz: Trueor False?
1. Asthma is an emotional or psychological illness
2. All people with asthma have allergies.
3. A number of Olympic medallists have asthma.
4. Asthma can be cured.
5. Children outgrow asthma.
6. A family history is a good predictor of whether or not a child
develops asthma.
7. Some dog beeds, such as chihuahuas, are better for people with
asthma and allergies.
8. All pet allergies will be cleared from a room once a pet is
removed.
9. Secondhand smoke may cause the development of asthma in
preschool children.
10. People with asthma should avoid all known asthma triggers.
65.
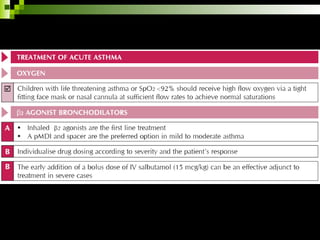
Management of acutesevere
asthma attack
Home management
Rescue medication inhaled short acting 2 agonist
Salbutamol Nebulization 1 ml = 5 mg
Three treatments in one hour or 4-8 puffs by inhaler/spacer
Response to initial Treatment is:
Good
Symptoms of subside and relief is sustained for 4 hours.
PEF is greater than 80%
Action
Continue 2 agonist every 3-4 hours for 1-2 days
66.
Incomplete
Symptoms decreasebut return in less than 3 hours
PEF is 60-80% predicted or personal best
Actions
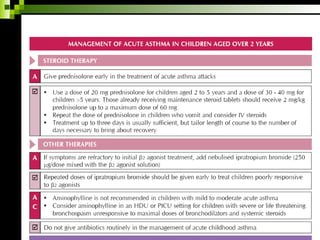
Add oral steriods
Add inhaled anticholinergic
Continue 2 agonist
Consult clinician urgently
Poor
PEF less than 60%
Transport to hospital emergency
67.
Hospital Management
Upon arrivalto emergency room after rapid
cardiopulmonary assessment:
Prompt Initiation of Oxygen therapy
Salbutamol Nebulization (3 back to back
treatments/ 4-8 puffs by inhaler/spacer)
Adrenaline s/c 0.01 mg/Kg can be used in
addition if no response
68.
Systemic glucocorticoid:Intravenous
methylprednisolone 1-2 mg/kg hydrocortisone
10mg/kg or IM route must be administered
Reassessment in 1 hour
If O2 saturation < 90, tachycardia shallow fast
breathing, altered sensorium admit PICU
69.
Continue O2
2 agonist inhalation every 20 minutes or continuous
Nebulization 0.5 mg/kg maximum 15 mg/hr
Anticholinergic Nebulization Ipratropium bromide 6
hourly
Intravenous fluids 2/3 maintenance
Intravenous Theophylline 6 mg/kg loading, 1 mg/kg
per hour
Intravenous Steroids
Intravenous 2 agonist 15 μg/kg over 15 min
If not improving and exhausted lethargic showing
increasing mixed acidosis
IV magnesium sulphate
ACUTE SEVERE ASTHMA
signs& symptoms
Cough
Sounds tight
Non-productive
Wheezing
Tachypnoea
Dyspnoea
Prolonged expiration
Use of accessory muscles of respiration
Cyanosis – hyperinflation
Tachycardia – pulsus paradoxas
72.
Extreme respiratorydistress
Silent chest
Wheezing comes after treatment
Difficulty walking or talking
Sitting up – hunched over
Abdominal pain
Liver
Spleen
Palpable
Vomiting
Sweating
Editor's Notes
#34 Classification of Asthmatics
Those who experience asthma associated with a cold that occurs from time to time are classified as intermittent. They are the group of asthmatics who we say grow out of the disease. They do not seem to be
bothered by asthma as they grow older.
Those having symptoms at least twice a week during the day or twice a month
during the night are classified as persistent.
































![Microsoft PowerPoint - Asthma 4th year Lecture (1) [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/microsoftpowerpoint-asthma4thyearlecture1compatibilitymode-220716165932-01cf3f8c-thumbnail.jpg?width=640&height=640&fit=bounds)
![Microsoft+PowerPoint+-+Asthma+4th+year+Lecture+(1)+[Compatibility+Mode].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/microsoftpowerpoint-asthma4thyearlecture1compatibilitymode-230704125445-487a63ed-thumbnail.jpg?width=640&height=640&fit=bounds)





















