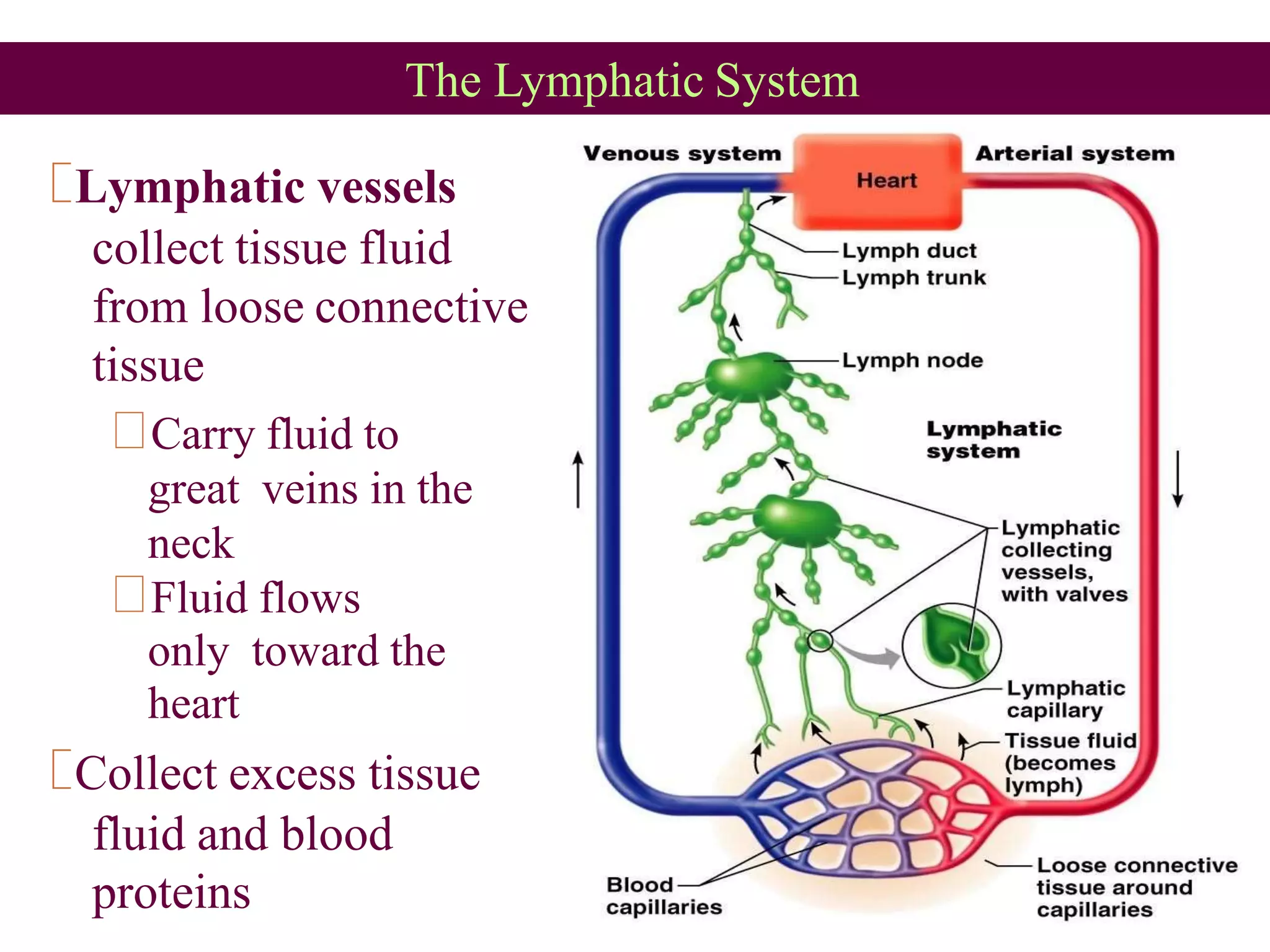
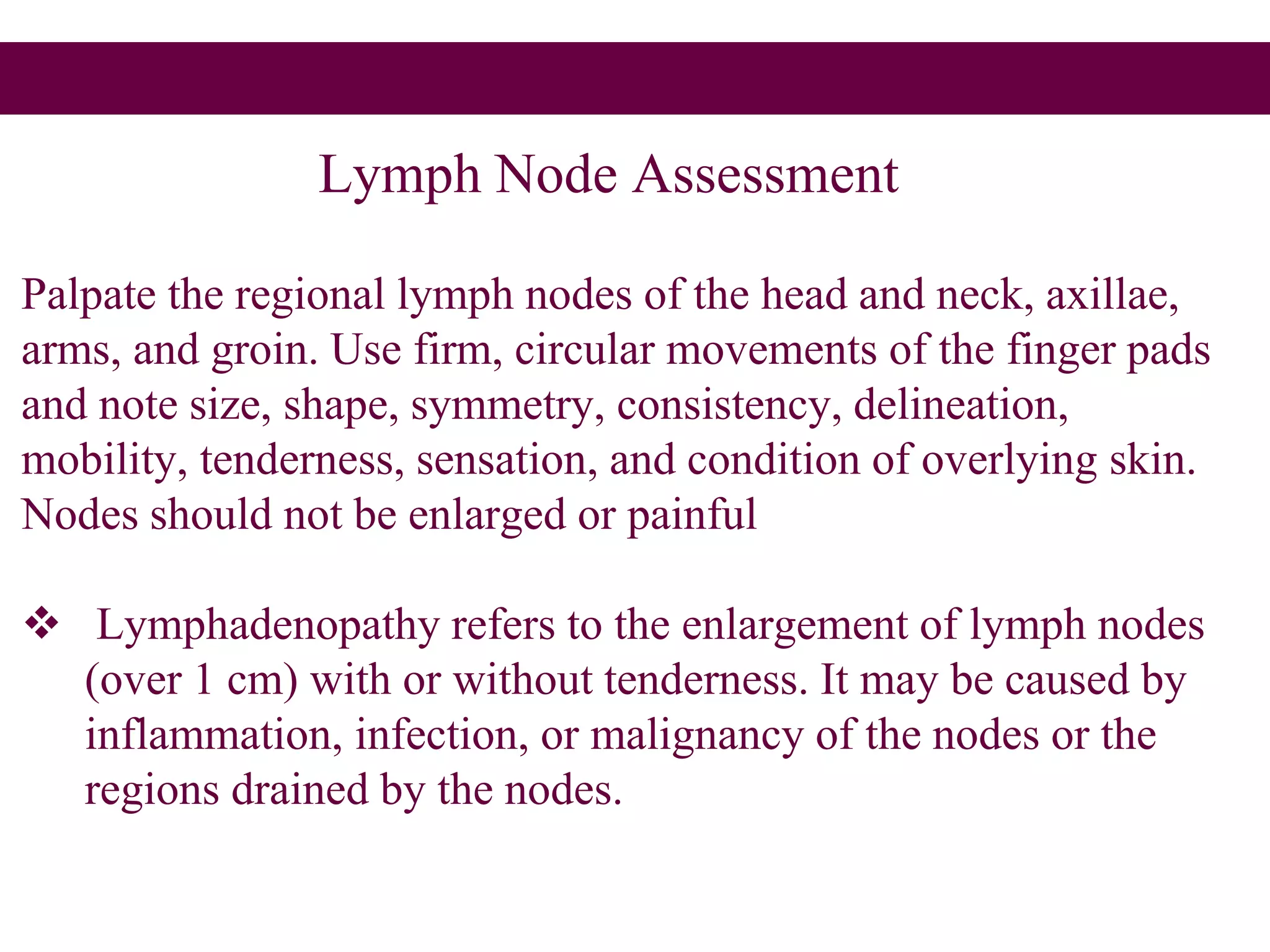
The lymphatic system transports fluid and immune cells throughout the body, removes cellular waste and pathogens, and presents antigens to immune cells. It consists of lymphatic vessels, lymph nodes, the spleen, thymus, tonsils, and bone marrow. Lymph fluid is collected from tissues by lymphatic capillaries and passes through lymph nodes, which filter the lymph and harbor immune cells. The lymph eventually returns to the blood circulation via lymph ducts in the neck. Enlargement of lymph nodes or spleen can indicate infection, inflammation, or cancer that is being assessed through history, exam, labs, and imaging.





















































![Hepatomegaly[1]](https://cdn.slidesharecdn.com/ss_thumbnails/hepatomegaly1-140726111452-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)


































![Lymphatic system [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/lymphaticsystemautosaved-180608144519-thumbnail.jpg?width=640&height=640&fit=bounds)






















