


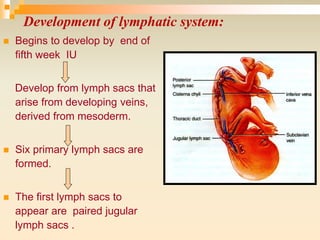
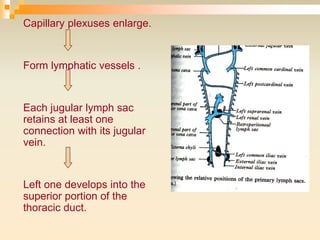
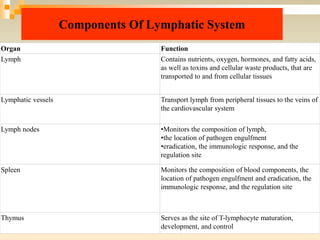


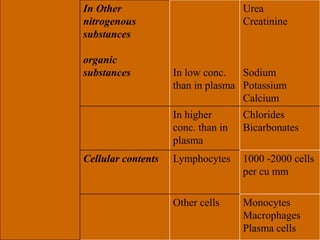
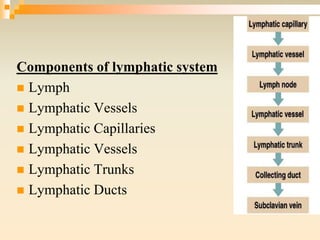



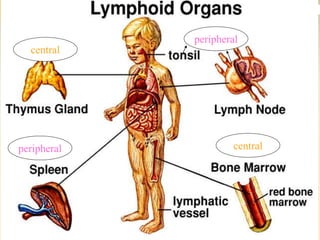
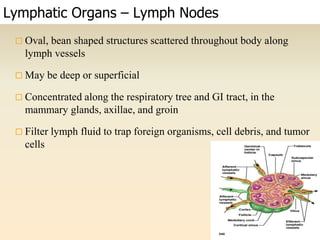


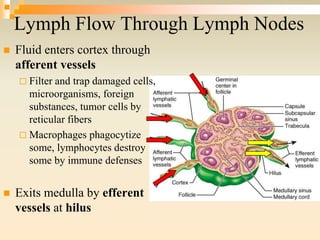
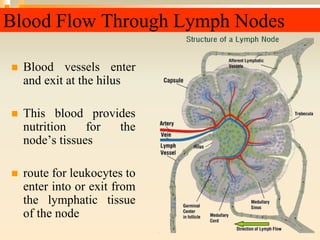































The lymphatic system consists of lymph, lymphatic vessels, lymph nodes, the spleen, thymus, and bone marrow. It develops from lymph sacs that arise from veins. The main functions are restoration of interstitial fluid, absorption and transport of fats, and defense against pathogens. Lymph contains nutrients, waste, and immune cells. It is transported through a network of vessels and ducts and emptied into subclavian veins. Lymph nodes filter lymph and activate immune cells to fight infection. The spleen, thymus, and bone marrow also participate in immune responses.



































































