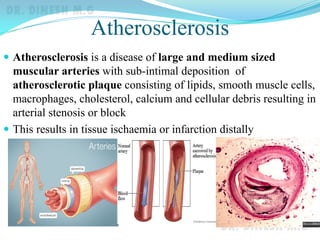
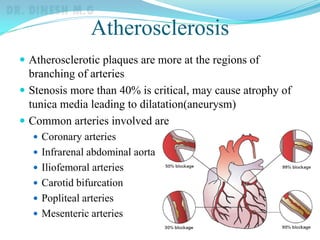
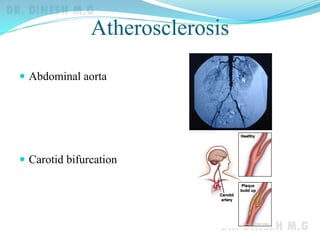
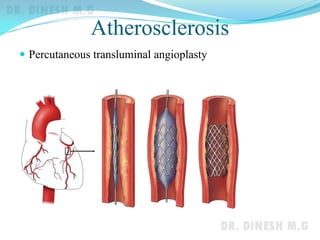
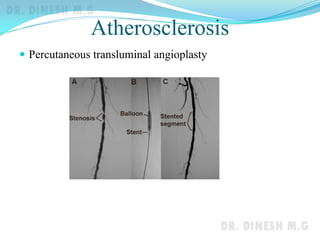
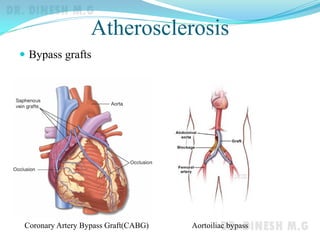
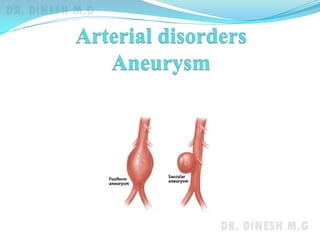
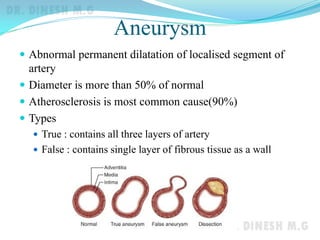
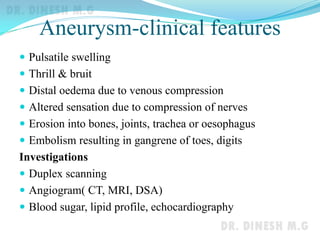
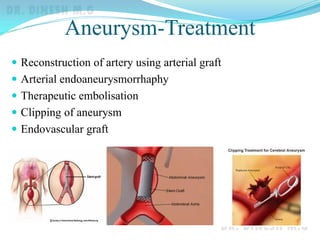
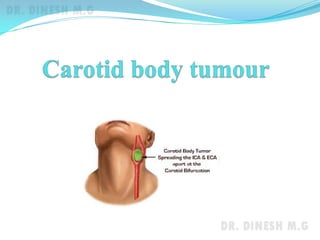
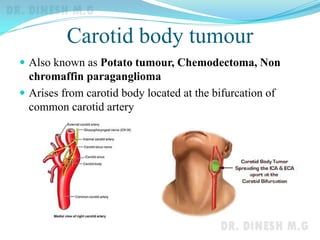
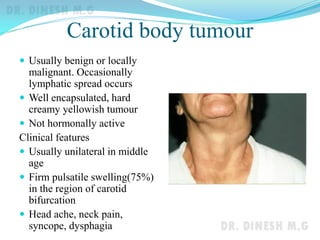
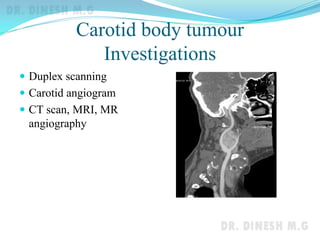
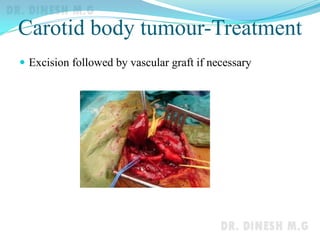

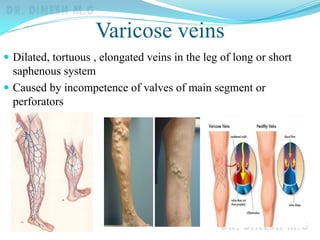


The document discusses atherosclerosis, aneurysms, carotid body tumors, and varicose veins. It defines each condition and describes their causes, risk factors, clinical features, investigations, and treatments. Atherosclerosis involves plaque buildup in arteries leading to narrowing or blockage and tissue ischemia. Treatments include risk factor modification, medications, angioplasty, surgeries like endarterectomy, and bypass grafts. Aneurysms are abnormal artery dilations over 50% in size caused mainly by atherosclerosis, with repair via open or endovascular grafting. Carotid body tumors are rare, usually benign growths at the carotid bifurcation treated by surgical excision. Varicose veins result




































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













