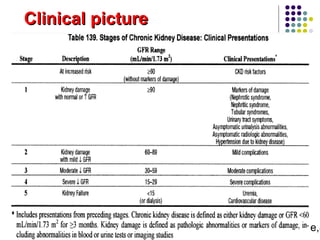
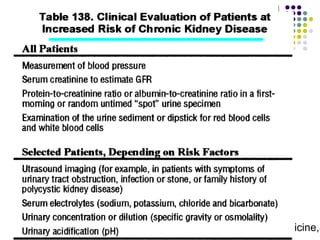
This document discusses chronic kidney disease (CKD). It defines CKD as a glomerular filtration rate below 60 mL/min/1.73m2 for over 3 months or evidence of kidney damage. CKD is classified into 5 stages based on GFR. Risk factors include diabetes, hypertension, and older age. Screening involves measuring creatinine and urine albumin levels. Treatment focuses on controlling blood pressure and diabetes to slow progression. Patients are referred to a nephrologist for advanced CKD stages, uncontrolled complications, or rapid decline in kidney function.
![DR.Basma M Abd El Aziz ,Family Medicine,S
Cockcroft-Gault equation :-
[[140 - age(yr)]*weight(kg)]/[72*serum Cr(mg/dL)]
(0.85 for women)
MDRD equation 7 :-
170 * [serum creatinine (mg/dL)]-0.999 * [age (years)]-
0.176 * [0.762 if pt is female] * [1.180 if pt is black] *
[BUN(mg/dL)]-0.170 * [albumin (g/dL)] +0.318
Equations for Estimating the GFR](https://image.slidesharecdn.com/approachtockd-170319050021/85/Approach-to-chronic-kidney-disease-8-320.jpg)
![DR.Basma M Abd El Aziz ,Family Medicine,S
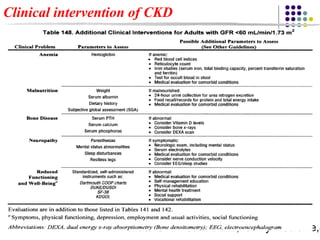
GFR is less than 30 mL per minute per 1.73 m2
severe cardiovascular disease.
Anemia of CKD
Bone and mineral disorder of CKD
Difficult to manage adverse effects of medications
Hyperkalemia (potassium level > 5.5 mEq per L [5.50 mmol per L] despite
treatment)
Refractory proteinuria (urinary protein/creatinine ratio > 500 to 1,000 mg per
g or urinary albumin/creatinine ratio > 300 mg per g)
Resistant hypertension (target blood pressure not achieved with use of at least
three antihypertensive drugs)
Stage 4 CKD (estimated GFR < 30 mL per minute per 1.73 m2)
Unexplained decrease in estimated GFR > 30 percent over four months
Indications for referral to a Nephrologist](https://image.slidesharecdn.com/approachtockd-170319050021/85/Approach-to-chronic-kidney-disease-30-320.jpg)














































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







