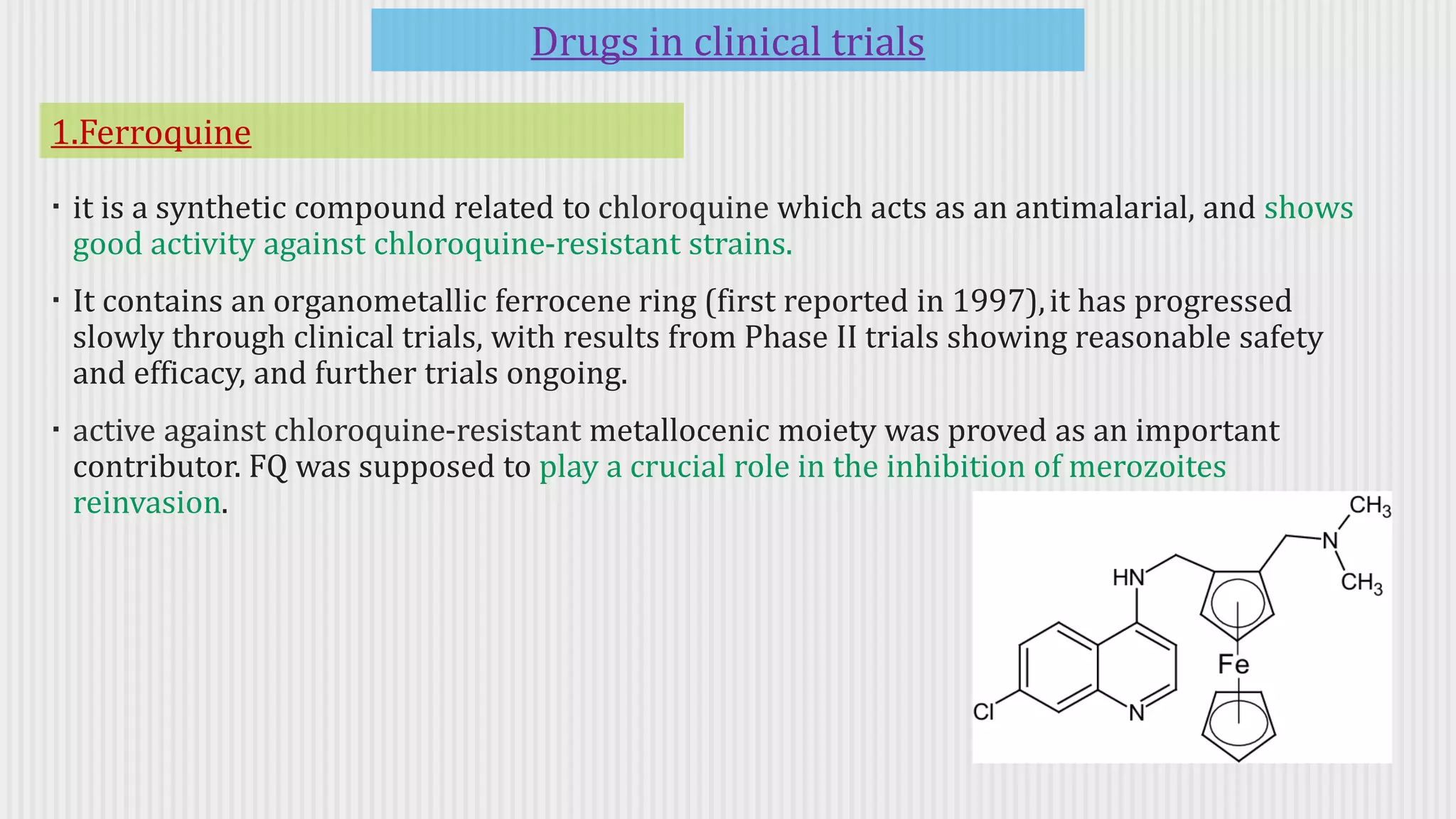
Srishti Bhargav presented an overview of anti-protozoal drugs. Many effective drugs are toxic and drug resistance is a major challenge. New drugs are needed with novel mechanisms of action. Several drugs discussed include paromomycin for giardiasis, piperaquine for malaria, posaconazole for fungal infections, and albaconazole which is in pre-clinical trials. Developing tools to detect resistance early and rational drug use and combinations can help address the threat of resistance in protozoal diseases.