Downloaded 19 times




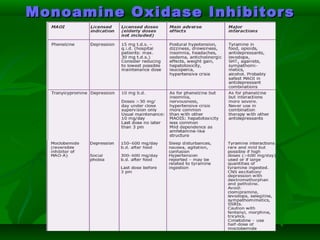
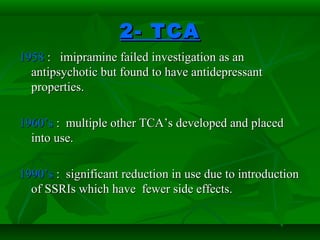
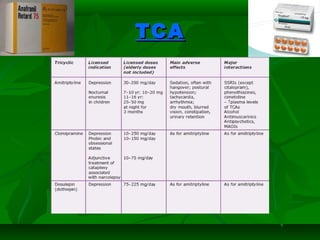
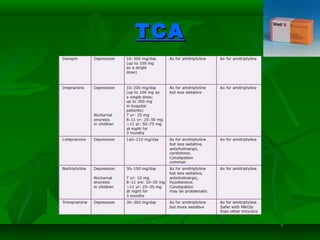

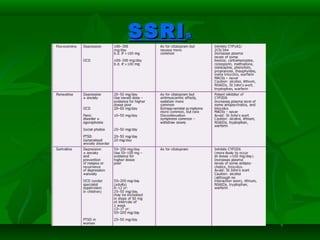
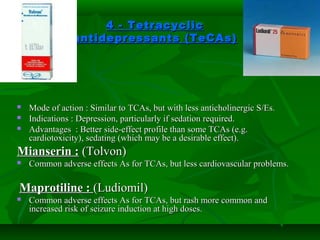


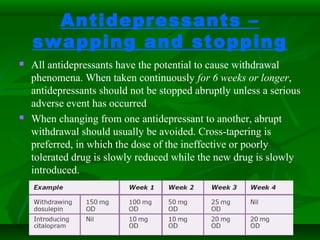



This document provides an overview of antidepressant drugs, including their history, classes, and clinical considerations. It discusses ten classes of antidepressants: monoamine reuptake inhibitors like TCAs, SSRIs, SNRIs, and NARIs; MAOIs; 5-HT2 receptor antagonists like mianserin and mirtazapine; NaSSAs like mirtazapine; NDRIs like bupropion; and St. John's wort. Each drug class is described in terms of its mode of action, indications, common adverse effects, advantages, and disadvantages. The document also lists antidepressants available on the Egyptian market.











































































































