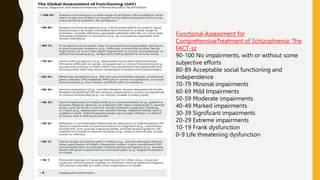
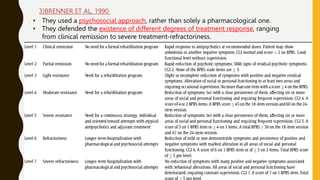
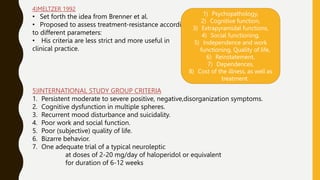
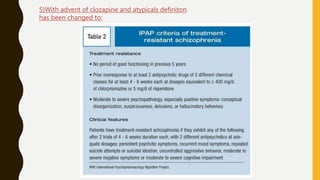
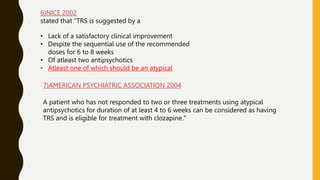
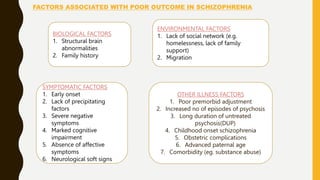
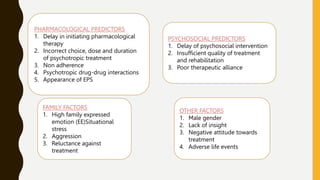
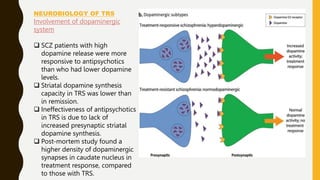
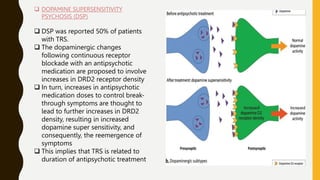
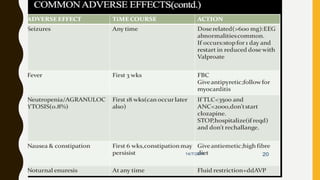
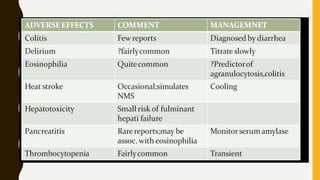
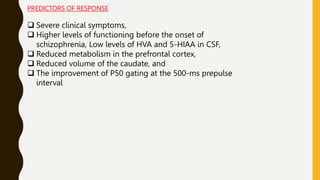
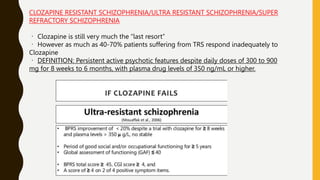
The document discusses treatment resistant schizophrenia, defining it as when patients do not respond to conventional antipsychotics or at least two different antipsychotics. It provides various definitions and criteria for treatment resistance proposed over time. It also discusses factors associated with poor outcomes in schizophrenia like biological, symptomatic, environmental, and illness factors. The neurobiology of treatment resistant schizophrenia is explained, involving the dopaminergic and glutamatergic systems. Evaluation of treatment resistant schizophrenia involves assessing patient factors, treatment factors, and conducting further investigations.