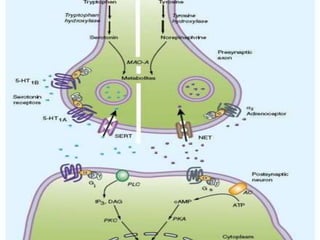
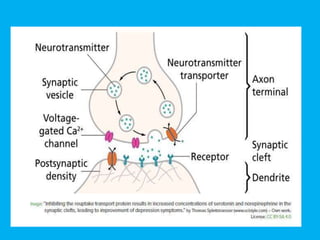
1. Antidepressants work by increasing levels of neurotransmitters like serotonin and norepinephrine in the brain. They are divided into several classes including SSRIs, SNRIs, TCAs, and MAOIs.
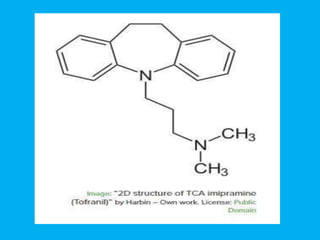
2. SSRIs are now the most commonly prescribed due to their safer side effect profile. They work by inhibiting reuptake of serotonin. TCAs affect serotonin and norepinephrine but have more side effects.
3. Antidepressants take 2-3 weeks to start working and should be taken long term to prevent relapse of depression. Side effects are usually mild and transient but can include nausea, sexual dysfunction, and dry mouth depending on the drug class.