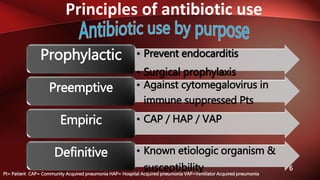
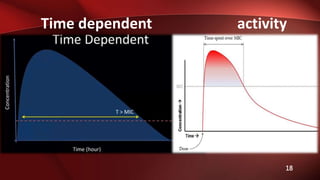
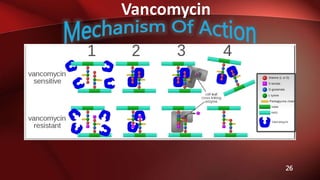
This document discusses principles of antibiotic use and optimization. It covers time dependent and concentration dependent antibiotic activity and mixed patterns. Prophylactic, preemptive, empiric and definitive antibiotic uses are defined. Vancomycin mechanisms of action, indications, dosing and adverse drug reactions are reviewed. Optimization includes appropriate dosing, duration, de-escalation and monitoring treatment response.
![Vancomycin
28
• Manufacturer’s labeling:
Usual dose: 500 mg every 6 hours or 1,000 mg
every 12 hours
• Alternate recommendations*:
15 to 20 mg/kg/dose every 8 to 12 hours
*(ASHP/IDSA/SIDP [Rybak, 2009]);](https://image.slidesharecdn.com/56c832d5-c49a-4fa8-a59e-00a64bb3a6b5-160209184624/85/Antibiotics-1-28-320.jpg)
![Vancomycin
29
• *Complicated infections in seriously ill
patients:
A loading dose of 25 to 30 mg/kg (based on
actual body weight)
*(ASHP/IDSA/SIDP [Rybak, 2009]);](https://image.slidesharecdn.com/56c832d5-c49a-4fa8-a59e-00a64bb3a6b5-160209184624/85/Antibiotics-1-29-320.jpg)