Download to read offline
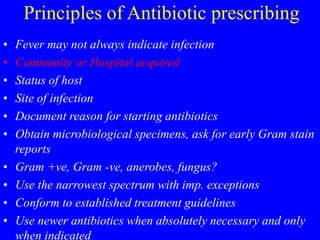


![Evolution of Antimicrobial Resistance
in Gram-Positive Cocci
S. aureus
Penicillin
[1940s] Penicillin-resistant
S. aureus
Methicillin
[1960s] Methicillin-resistant
S. aureus (MRSA)
Vancomycin-resistant
enterococcus (VRE)
Vancomycin
[1997]
Vancomycin
(glycopeptide)
intermediate-resistant
S. aureus
Vancomycin-
resistant
S. aureus
Ciprofloxacin
1987
[2002]
Adapted from: CDC. Prevent Antimicrobial Resistance: A Campaign for Clinicians. April 2002.](https://image.slidesharecdn.com/antibioticprinciples-230313133344-03f1123f/85/antibiotic-principles-ppt-22-320.jpg)
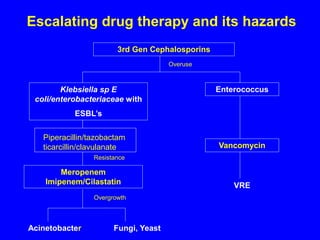
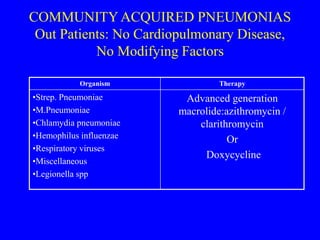
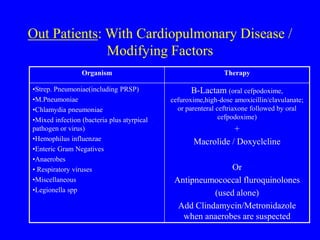
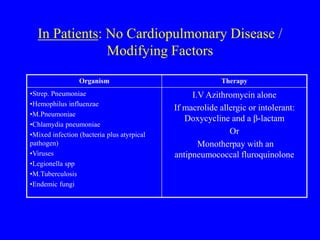
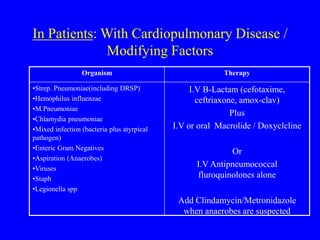


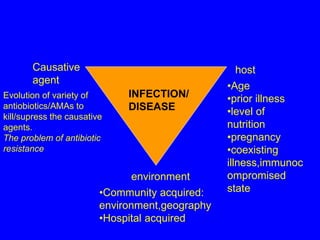
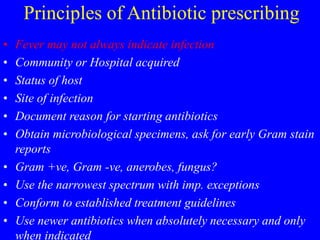
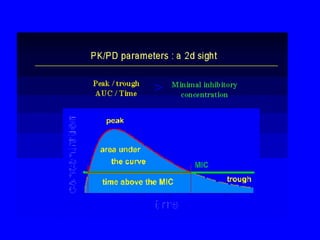
This document discusses principles of antibiotic therapy and treatment of infections. It covers: - Factors that influence infection like the host, environment, and causative agent - Principles of antibiotic prescribing including obtaining cultures, using the narrowest effective spectrum, and conforming to treatment guidelines - The growing problem of antibiotic resistance due to overuse and misuse of antibiotics - Examples of optimal treatment for different types of infections like community-acquired pneumonia, bone infections, and skin/soft tissue infections





























![Antibiotic therapy in the intensive care unit [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/antibiotictherapyintheintensivecareunitautosaved-141106103023-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)


















![Balanced Crystalloids Webinar February 2023[2207].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/balancedcrystalloidswebinarfebruary20232207-240501141244-58dce968-thumbnail.jpg?width=640&height=640&fit=bounds)



![Traumatic brain injury [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/traumaticbraininjuryautosaved-230313134042-a66a1551-thumbnail.jpg?width=640&height=640&fit=bounds)























