![SUBMITTED TO: SUBMITTED BY:
DR. PALLAVI PATHANIA MS. SABNAM KUMARI
ASSOCIATE PROFESSOR M.Sc. [N] 1ST YEAR
SHIMLA NURSING COLLEGE SHIMLA NURSING COLLEGE
Presentation
on
anatomy and physiology of
the skin](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Anatomy and physiology of skin .pptx
Similar to Anatomy and physiology of skin .pptx (20)
Recently uploaded
Recently uploaded (20)
Anatomy and physiology of skin .pptx
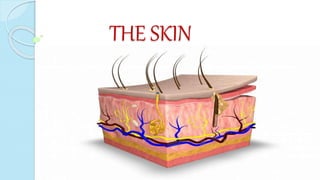
- 1. THE SKIN
- 2. SUBMITTED TO: SUBMITTED BY: DR. PALLAVI PATHANIA MS. SABNAM KUMARI ASSOCIATE PROFESSOR M.Sc. [N] 1ST YEAR SHIMLA NURSING COLLEGE SHIMLA NURSING COLLEGE Presentation on anatomy and physiology of the skin
- 3. INDEX SR.NO. CONTENT 1. Introduction of Integumentary system 2. Introduction about skin 3. Definition 4. Layers of skin
- 4. SR. NO. CONTENT 4. Epidermis 5. Dermis Blood and lymph vessels Sensory and nerve endings Sweat glands Sebaceous glands Hairs Nails
- 5. SR . NO. CONTENT 6. Subcutaneous layer 7. Functions of skin 8. Disorders of skin • viral infections Human papilloma Herpes virus Prevention of viral infection • Bacterial infections Impetigo Candidiasis Cellulitis Prevention of bacterial infection
- 6. SR.NO. CONTENT • Fungal infection Ringworm Tinea Pedis Prevention of fungal infection • Non- infective inflammatory conditions Dermatitis Atopic dermatitis Contact dermatitis Psoriasis Acne vulgaris • Burns •Prevention and management of burns • Pressure ulcers (Decubitus ulcers) Prevention of pressure ulcers
- 7. SR.NO. CONTENT • Malignant tumors Basal cell carcinoma Malignant melanoma Kaposi’s sarcoma Prevention of malignant disorders •Conclusion •Summary •Recapitalization
- 8. INTEGUMENTARY SYSTEM: Integumentary- coverings: covers outside of the body. It comprises the skin and its appendages, acting as a physical barrier between the external environment and the internal environment that it serves to protect and maintain.
- 9. INTEGUMENTARY SYSTEM CONSISTS Skin and appendages Nails Hair Follicles Skin Glands
- 10. STRUCTURE OF THE SKIN
- 11. The skin, also known as cutis or integument that serves as main covering of the body. The skin is the largest organ of the body weighing up to 16% of total body weight. For the average adult human, the skin has a surface area of between 1.5-2.0 sq.meters. Thickness:0.5 to 3mm.
- 12. The body’s basic defense covering, which protects against heat and light, injury and infection. The skin completely covers the body and is continuous with the membranes lining the body orifices.
- 13. LAYERS OF SKIN Epidermis Dermis Hypodermis(Subcutaneous layer)
- 15. EPIDERMIS
- 16. THE EPIDERMIS The epidermis is the outermost layer of the skin. The epidermis is composed of the keratinized squamous epithelium and does not have a blood supply of its own.
- 18. LAYERS OF EPIDERMIS It is made up of five layers: Stratum corneum Stratum lucidum Stratum granulosum Stratum spinosum Stratum germinativm
- 19. LAYERS OF EPIDERMIS Stratum corneum- The outer most layer of the skin. This is made up of scale like cells that are continuously shed. Stratum lucidum- This is made up of small transparent cells through which light can pass. This layer only present in the palms of hands and soles. Stratum granulosum- This layer is usually 1-3 layers thick. The cells have distinct granules and keratin is produced in the layer.
- 20. Stratum spinosum- This layer is 3-6 layers thick and the cells are constantly dividing. Stratum germinative- A single basal layer of cells, which contain the melanocytes that produce the produce the pigment melanin. The cells of the epidermis are produced in the layer and each has a distinct nuclei. These cells divide continuously by a process known a mitosis.
- 21. STRATUM GERMINATUM CONTAINS MELANIN The melanocytes produce extra melanin when activated by UV rays, however they sometimes hyper-secrete resulting in hyper- pigmentation i.e. darker patches of skin color. If the melanocytes hypo secrete or cease to secrete melanin hypo pigmentation occurs, this skin condition is referred to as vitiligo.
- 22. DERMIS
- 23. INTRODUCTION DERMIS The layer is often referred to as the true skin as it forms the bulk of the skin. The dermis has a good blood and lymph supply provided by lymph capillaries, arterioles and venules. It is tough and elastic.
- 24. CONTINUED The dermis is made up of connective tissue, and the matrix contains collagen fibers interlaced with the elastic fibre.
- 25. LAYERS OF DERMIS PAPILLARY LAYER RETICULAR LAYER
- 26. LAYERS OF DERMIS PAPILLARY LAYER Lies directly under the epidermis, it is quite thin and has cone like projections called papillae. It provides nutrients and oxygen to the germinating layer of the epidermis.
- 27. RETICULAR LAYER This lies below the papillary layer and is the main section of the dermis. Within the reticular layer collagen and elastin fibers are present.
- 28. RETICULAR LAYER CONSIST OF: COLLAGEN Collagen gives the skin plump and youthful appearance and is a white fibrous tissue made up of proteins. Collagen fibers bind water and give the skin its tensile strength, but as this ability declines with age, wrinkles develop.
- 29. CONTINUED ELASTIN Elastin gives the skin its elastic properties and is made up of yellow elastic tissue. Rupture of elastic fibers occurs when the skin is overstretched, resulting in permanent striae, or stretch marks, which are typically found in pregnancy and obesity.
- 30. STRUCTURES FOUND IN DERMIS Small blood and lymph vessels. Sensory nerve endings. Sweat glands and their ducts. Hairs, arrector pilli muscles and sebaceous glands..
- 31. STRUCTURES FOUND IN DERMIS BLOOD AND LYMPH SUPPLY Blood is supplied to the skin by small blood vessels known as blood capillaries. Arterioles form a fine network with capillary branches supplying sweat glands, sebaceous glands, hair follicles and the dermis.
- 32. CONTINUED BLOOD AND LYMPH VESSELS Arterioles supply oxygenated blood that is rich in nutrients and venules remove waste products and carbon dioxide. In addition, the capillaries also help to maintain the body temperature by dilating and constricting. Lymph vessels also form a network throughout the dermis.
- 33. CONTINUED SENSORY NERVE ENDINGS Sensory receptors (specialized nerve endings) sensitive to touch, temperature, pressure, and pain are widely distributed in the dermis. Nerve impulses, generated in the sensory receptors in the dermis, are transmitted to the spinal cord by sensory nerves. From there, impulses are conducted to the sensory area of the cerebrum, where the sensations are perceived.
- 34. CONTINUED SENSATIONS SENSORY RECEPTORS Touch Meissners corpuscles Pain Pain corpuscles Pressure Pacinain corpuscles Heat Ruffins end corpuscles Cold Krauses end bulb
- 35. STRUCTURES FOUND IN DERMIS SWEAT GLANDS The Sweat glands ,which are sometimes referred to as the sudoriferous glands. Derived from Latin word sudor 'sweat', are small tubular structures of the skin that produce sweat.
- 36. CONTINUED SWEAT GLANDS Sweat glands are appendages of the Integumentary system. They extend from the epidermis into the dermis and are found all over the body, however they are particularly numerous in the palms of the hands and the soles of the feet. They regulate the body temperature by allowing sweat to evaporate from the body.
- 37. TYPES OF SWEAT GLAND ECCRINE GLANDS APPOCRINE GLANDS
- 39. TYPES OF SWEAT GLANDS ECCRINE GLANDS These are the more common types of sweat glands and open on to the skin surface through tiny pores. Found all over the body surface and secrete in response to heat. When the internal temperature of the body rises, sweat glands release water to the skin surface. There, it quickly evaporates, subsequently cooling the skin and blood beneath.; this is the most effective means of thermoregulation in humans. Eccrine sweat glands also participate in ion and nitrogenous waste excretion.
- 40. CONTINUED APOCRINE GLANDS: Larger and deeper glands found in the groin and underarm regions. These glands are under hormonal control and play a role in sexual arousal. These glands are open into hair follicles and therefore become active at puberty. The apocrine glands produce sweat that decays to produce an unpleasant odor.
- 41. EXAMPLE OF APOCRINE GLAND They are large, branched glands, mostly confined to the axillary and perineal regions, including the perineal region, labia majora in women, and the scrotum and prepuce in men. Apocrine sweat glands are also present in the nipples and areola tissue surrounding the nipples. Modified apocrine sweat glands include the wax-producing ceremonious glands of the external auditory meatus, the Moll glands found at the free margins of the eyelids, and the mammary glands of the breast.
- 42. THE HAIR
- 43. THE HAIR Hair are dead structures that are made up of a hardened protein called keratin. Keratin provides the body with a protective toughness for its entire surface.
- 44. THE HAIR FOLLICLE The hair follicle is a tunnel- shaped structure in the epidermis of the skin. Hair starts growing at the bottom of a hair follicle.
- 45. PARTS OF HAIR SHAFT Portion of hair that lies above the skin surface, but also runs through the centre of the hair. ROOT Portion of hair that lies underneath the skin, inside the follicle.
- 46. CONTINUED BULB Is the large base at the bottom of the root and it encases the dermal papilla. The matrix is the lower region of the bulb where the cells divide rapidly to produce the new hair and follicle structure.
- 47. LAYERS OF HAIR Cuticle Cortex Medulla
- 48. Cuticle: Thin protective outer layer that contains the nourishing portion essential to hair growth. It is highly keratinized, composed of cells shaped like scales that are layered one over the other, measuring about 60 micrometers long and about 6 micrometer wide.
- 49. CONTINUED Cortex: It forms the main bulk and pigment(color) of the hair. It consists of long keratin filaments. Medulla: innermost layer of the hair shaft, composed of an amorphous, soft, oily substance.
- 50. ARRECTOR PILI MUSCLES The muscle is attached to the hair follicle and it contracts when one feels cold or gets frightened and in result the hairs get erect. This is stimulated by sympathetic nerve fibers in response to fear and cold. Erect hair traps air, which acts as an insulating layer, providing an efficient warming mechanism, especially when accompanied by shivering.
- 51. SEBACEOUS GLAND Secretory glands consist of secretory epithelial cells derived from the same tissue as the hair follicles. These glands are found all over the body except for the palms of the hands and the soles of the feet and produce the natural oil of the skin- sebum. They are most numerous in the scalp, face, axillary and groin region.
- 52. CONTINUED In regions of transition from one type of superficial epithelium to another such as lips, eyelids, nipple, labia minora and glans penis, therefore they are sebaceous glands that are independent of hair follicles, secreting sebum directly on the surface. SEBUM: Sebum is the bactericidal and fungicidal and so prevents against infection, it also provides protection and prevents the skin from drying out.
- 53. THE NAIL
- 54. INTRODUCTION The nails are the extension of the epidermis and are therefore an appendages of the skin. They are required to help with grasping and protect the fingertip and toes. The root of nail is embedded in the skin and covered by the cuticle, which forms the hemispherical pale area called the lunula.
- 55. STRUCTURES OF NAIL The structures that define and produce the nail (nail plate) include the matrix (sterile and germinal), the eponychium (thickened layer of skin at the base of finger nails and toe nails), the paronychium (para- next, onyx- nail i.e. next to nail), and the hyponychium (skin just under the free edge of the nail).
- 56. CONTINUED Collectively, the nail bed (sterile matrix), nail fold, eponychium, paronychium, and hyponychium are referred to as the perionychium.
- 57. ABNORMALITIES OF NAIL BEAU’S LINE Depressions that run across your fingernail are called beau’s lines. These can be a sign of malnourishment.
- 58. CLUBBING Clubbing is when your nails thicken and curve around your fingertips, a process that generally takes years. This can be the result of low oxygen in the blood and is associated with: cardiovascular diseases Inflammatory bowel disease Liver diseases
- 59. KOLIONYCHIA (SPOONING ) Koilonychia is when your fingernails have raised ridges and scoop outward, like spoons. It’s also called “spooning.” Sometimes the nail is curved enough to hold a drop of liquid. Spooning can be a sign that you have: iron deficiency anemia heart disease Hemochromatosis, a liver disorder that causes too much iron to be absorbed from food.
- 60. LEUKONYCHIA Non-uniform white spots or lines on the nail are called leukonychia. They usually the result of a minor trauma and are harmless in healthy individuals. Sometimes leukonychia is associated with poor health or nutritional deficiencies.
- 61. MEES LINES Mees lines are transverse white lines. This can be a sign of arsenic poisoning. If you have this symptom, your doctor will take hair or tissue samples to check for arsenic in your body.
- 62. PITTING Pitting refers to small depressions, or little pits, in the nail. It’s common in people who have psoriasis, a skin condition that causes the skin to be dry, red, and irritated. Some systemic diseases can also cause pitting.
- 63. TERRY’S NAILS When the tip of each nail has a dark band, it’s called Terry’s nails. This is often due to aging, but it can also be caused by: Congestive heart failure Diabetes Liver disease
- 64. YELLOW NAIL Yellow nail syndrome is when the nails get thicker and don’t grow as fast as normal. Sometimes the nail lacks a cuticle and may even pull away from the nail bed. This can be the result of: Internal malignancies Lymphedema, swelling of the hands. Pleural effusions, fluid buildup between the lungs and chest cavity.
- 65. EFFECT OF CHEMOTHERAPY ON NAIL COLOR Your nails may look bruised — turning black, brown, blue, or green. People with darker complexions notice the color change more. You may develop blemishes on your nails such as a horizontal or vertical line, or small indentations. Your nails may become thin or brittle. The nail can lift completely off the nail bed or fall off in some cases.
- 66. FUNCTIONS OF NAIL Nails protect the sensitive tips of fingers and toes. They also protect the fingers and toes from injury. They help us to pick up small objects. The matrix creates new skin cells, which pushes out the old, dead skin cells to make your nails.
- 68. SUBCUTANEOUS LAYER This is located under the dermis and is mainly made up of fat cells (adipose tissue). This fatty layer provides the plump contours of the body, protection, insulation, support and nutrients supply if needed.
- 69. FUNCTIONS OF SKIN Sensation Heat regulation Absorption Protection Excretion Secretion Vitamin D production
- 71. VIRAL INFECTIONS HUMAN PAPILLOMA VIRUS Human papillomavirus (HPV) is a viral infection that's passed between people through skin-to-skin contact. Common sites are the hands, the face and the soles of the feet. CAUSE- HPV SYMPTOMS- Common warts, plantar warts, and flat warts.
- 72. HUMAN PAPILLOMA VIRUS DIAGNOSIS History collection, Physical examination, Pap smear, Colposcopy. TREATMENT HPV vaccine, Salicylic acid, Imiquimod, Trichloroacetic acid.
- 73. CONTINUED HERPES VIRUSES Herpes is an infection that is caused by a herpes simplex virus (HSV). Oral herpes causes cold sores around the mouth or face. Genital herpes affects the genitals, buttocks or anal area. Genital herpes is a sexually transmitted disease (STD).
- 74. HERPES SIMPLEX VIRUS CAUSE- Herpes simplex virus SYMPTOMS Blistering sores (in the mouth or on the genitals), Pain during urination (genital herpes), Itching fever, Swollen lymph nodes, Headaches, Tiredness, Lack of appetite. DIAGNOSIS History collection , Physical examination, Swab test, Blood test, Lumbar puncture. TREATMENT Acyclovir, Famciclovir.
- 75. PREVENTION Wash your hands with soap and warm water frequently. Avoid sharing eating utensils and drinking glasses with other people. Avoid direct contact with the skin of other people who have an infection. Consult your dermatologist.
- 76. BACTERIAL INFECTIONS IMPETIGO This is a highly infectious condition. It is spread by direct contact and affects mainly children and immunosuppressed individuals. CAUSE- Staphylococcus aureus SYMPTOMS Superficial pustules develop, usually round the nose and mouth, pruritis, fever.
- 77. IMPETIGO DIAGNOSIS History collection, Physical examination, Blood test. TREATMENT Antibiotic ointment mupirocin (Bactroban), Penicillin drug, Cephalexin.
- 78. CONTINUED CELLULITIS This is a spreading infection, which enter through a break in the skin. Cellulitis usually affects the skin on the lower legs, but it can occur in the face, arms and other areas CAUSES- caused by some anaerobic bacteria, including streptococcus pyogenes and clostridium perfringens. .
- 79. CELLULITIS SYMPTOMS Red area of skin that tends to expand, Swelling, Tenderness, Pain, Warmth, Fever, Red spots, Blisters, Skin dimpling. DIAGNOSIS History collection, Physical examination, Blood test, Bacterial culture. TREATMENT Dicloxacillin, Cephalexin, Trimethoprim with sulfamethoxazole, Clindamycin.
- 80. PREVENTION Avoid touching your eyes, nose, or mouth with your hands to help prevent the spread of infections. Do not squeeze skin sores, it may worsen the infection and possibly spread it to others. Completely and securely cover skin infections that are not contagious (such as eczema) before practice, meets, or games. Wash hands frequently. Consult your dermatologist.
- 81. FUNGAL INFECTION (MYCOSES) RINGWORM Ringworm is a contagious fungal infection caused by common mold-like parasites that live on the cells in the outer layer of your skin. Also known as tinea or dermatophytosis Ringworm often spreads by direct, skin-to-skin contact with an infected person.
- 82. MODE OF TRANSMISSION It get transmitted from an- Infected person Animal Inaminate object Soil
- 83. TYPE OF RINGWORM Ringworm that affect the- 1. Skin(Tinea corporis) 2. Scalp(Tinea capitis) 3. Feet (Tinea pedis or athlete’s foot 4. Nail(Tinea Unguium) 5. Face( Tenia Faciei) 6. Beard Area( Tenia Barbae) 7. Hans And palm areas9 Tinea manuum)
- 84. RING WORM Symptoms:- Itchy, ring shaped scaly patches that may blister, hair loss, Dandruff or seborrhea Diagnostic evaluation:- Skin biopsy Management:- Clotrimazole, miconazole
- 85. FUNGAL INFECTION CANDIDIASIS Candidiasis is a fungal infection caused by a yeast (a type of fungus) called Candida. Candida normally lives on the skin and inside the body, in places such as the mouth, throat, gut, and vagina, without causing any problems. CAUSE- most common cause is Candida albicans.
- 86. CANDIDIASIS SYMPTOMS Oral Thrush, tiredness and fatigue, Recurring Genital or Urinary Tract Infections, Sinus Infections, joint pain, Skin and Nail Fungal Infections. DIAGNOSIS History collection, Physical examination, Blood test, culture. TREATMENT Fluconazole, Clotrimazole.
- 87. CONTINUED TINEA PEDIS Athlete's foot (tinea pedis) is a fungal infection that usually begins between the toes. It commonly occurs in people whose feet have become very sweaty while confined within tight fitting shoes. Signs and symptoms of athlete's foot include a scaly rash that usually causes itching, stinging and burning.
- 88. TINEA PEDIS CAUSE- Tinea pedis SYMPTOM Athlete's foot may appear as pink-to-red skin, Pain, Itchy blisters on the arch (instep) and/or the ball of the foot. DIAGNOSIS History collection, Physical examination, Potassium hydroxide exam. TREATMENT Luliconazole, an imidazole topical cream.
- 89. PREVENTION Keep your skin clean and dry, particularly the folds of your skin. Wash your hands often, especially after touching animals or other people. Avoid using other people's towels and other personal care products. Wear shoes in locker rooms, community showers, and swimming pools. Consult your dermatologist.
- 90. NON- INFECTIVE INLAMMTORY CONDITIONS DERMATITIS (ECZEMA) Dermatitis is a common inflammatory skin condition that may either acute or chronic. CAUSE- allergic reaction to: Detergents, Cosmetics, Nickel, Stress, hormonal changes.
- 91. CONTINUED SYMPTOMS In acute dermatitis there is redness, swelling and exudation of serous fluid, usually accompanied by pruritis (itching), crusting or scaling. In chronic condition the skin become thickens and may become leathery due to long- term scratching, which may cause infection.
- 92. CONTINUED ATOPIC DERMATITIS (ECZEMA) It is a condition that makes your skin red and itchy. It's common in children but can occur at any age. Atopic dermatitis is long lasting (chronic) and tends to flare periodically. It may be accompanied by asthma or hay fever.
- 93. CONTINUED CONTACT DERMATITIS This is caused by direct contact with irritants, e.g. cosmetics, soap, detergent, strong acids or alkalis, industrial chemicals or a hypersensitivity reaction to latex nickel, dyes and other chemicals.
- 94. CONTINUED DIAGNOSIS History collection Physical examination Patch test TREATMENT Antihistamine such as diphenhydramine (Benadryl) Phototherapy Hydrocortisone, to relieve itchiness and inflammation. Creams or lotions for dry skin.
- 95. CONTINUED PSORIASIS Psoriasis is thought to be an immune system problem. Triggers include infections, stress and cold. Psoriasis is a common, long-term (chronic) disease. CAUSE Infections, such as strep throat or skin infections, Weather, especially cold, dry conditions, Injury to the skin, such as a cut or scrape, a bug bite, or a severe sunburn, Smoking.
- 96. PSORIASIS SYMPTOMS Psoriasis is a skin disease that causes red, itchy scaly patches, most commonly on the knees, elbows, trunk and scalp. DIAGNOSIS History collection, Physical examination, Skin biopsy. TREATMENT Vitamin D analogues, Corticosteroids, Salicylic acid.
- 97. CONTINUED ACNE VULGARIS Acne vulgaris is a common chronic skin disease involving blockage and/or inflammation of pilosebaceous units (hair follicles and their accompanying sebaceous gland). Acne can present as non inflammatory lesions, inflammatory lesions, or a mixture of both, affecting mostly the face but also the back and chest.
- 98. ACNE VULGARIS CAUSE Excess oil (sebum) production, Hair follicles clogged by oil and dead skin cells, Bacteria, Hormonal changes in pregnancy or from the menstrual cycle. SYMPTOMS Whiteheads (closed plugged pores), Blackheads (open plugged pores), Small red, tender bumps (papules), Pimples (pustules), which are papules with pus at their tips, Large, solid, painful lumps under the skin (nodules), Painful, pus-filled lumps under the skin (cystic lesions).
- 99. ACNE VULGARIS DIAGNOSIS History collection, Physical examination, Swab test. TREATMENT Topical antibiotics- benzyl peroxide or a topical retinoid. Oral antibiotics- doxycycline and minocycline
- 100. PREVENTION Avoid contact with irritants and allergens. Wear protective clothing or gloves. Apply a barrier cream or gel for e.g. sunscreen. Avoid excessive exposure to direct sunlight. Consult your dermatologist.
- 101. PRESSURE ULCERS (DECUBITUS ULCERS) Pressure ulcers (also known as pressure sores or bedsores and decubitus ulcers) are injuries to the skin and underlying tissue, primarily caused by prolonged pressure on the skin. They can happen to anyone, but usually affect people confined to bed or who sit in a chair or wheelchair for long periods of time.
- 103. CONTINUED CAUSE Caused by sustained pressure being placed on a particular part of the body. SYMPTOMS Part of the skin becoming discolored – people with pale skin tend to get red patches, while people with dark skin tend to get purple or blue patches, Pain or itchiness in the affected area. DIAGNOSIS History collection, Physical examination, Braden scale.
- 104. CONTINUED TREATMENT Removing pressure on the affected area. Protecting the wound with medicated gauze or other special dressings. Keeping the wound clean. Ensuring good nutrition. Removing the damaged, infected, or dead tissue (debridement). Transplanting healthy skin to the wound area (skin grafts). Negative pressure wound therapy. Medicine (such as antibiotics to treat infections).
- 106. PREVENTION Perform skin assessments every 8 hours using the Braden Scale. Reposition the patient every 2 hour to offload pressure using a pillow or wedge. Ensure adequate nutritional status to improve wound healing. Maintain adequate hydration.
- 107. BURNS Burns are tissue damage that results from heat, overexposure to the sun or other radiation, or chemical or electrical contact. Burns can be minor medical problems or life-threatening emergencies. CAUSE- Hot fluids Excessive exposure to radiation Chemical burn
- 108. CONTINUED SYMPTOMS Swelling and red, white or splotchy skin. Blisters may develop, and pain can be severe. Deep second-degree burns can cause scarring. DIAGNOSIS History collection Physical examination Rule of nine Parkland formula
- 109. Cool the burn. Hold the burned area under cool (not cold) running water or apply a cool, wet compress until the pain eases. Assess degree of burn. Remove rings or other tight items. Don't break blisters. Bandage the burn. Take a pain reliever. Fluid and electrolytes replacement should be done. Apply silver sulfadiazine over the burn area. Plastic surgery, skin grafting. TREATMENT
- 110. PREVENTION Be “alarmed”. Install and maintain smoke alarms in your home—on every floor and near all rooms family members sleep in. Have an escape plan. Create and practice a family fire escape plan, and involve kids in the planning. Cook with care. Check water heater temperature.
- 111. MALIGNANT TUMORS BASAL CELL CARCINOMA Basal cell carcinoma is a type of skin cancer that most often develops on areas of skin exposed to the sun. Basal cell carcinoma is a type of skin cancer. CAUSE- Excessive exposure to sunlight, Radiation therapy, increased age, immunosuppressive therapy.
- 112. CONTINUED SYMPTOMS A pearly white, skin-colored or pink bump, A brown, black or blue lesion, A flat, scaly, reddish patch, white, waxy, scar-like lesion. DIAGNOSIS History collection, Physical examination, TNM classification, Biopsy. TREATMENT Chemotherapy, Radiation therapy, Mohs surgery, Topical ointment.
- 113. CONTINUED MALIGNANT MELANOMA Melanoma, also redundantly known as malignant melanoma, is a type of skin cancer that develops from the pigment-producing cells known as melanocytes. Melanomas typically occur in the skin but may rarely occur in the mouth, intestines or eye (uveal melanoma).
- 114. CONTINUED CAUSES Excessive exposure to UV radiation, Genetics SYMPTOMS Asymmetry, Borders (irregular with edges and corners), Color (variegated), Diameter (greater than 6 mm, about the size of a pencil eraser), Evolving over time. DIAGNOSIS History collection , Physical examination, Biopsy, TNM staging. TREATMENT Chemotherapy, Immunotherapy, Tumor resection.
- 115. KAPOSI’S SARCOMA It is a type of cancer that forms in the lining of blood and lymph vessels. The tumors (lesions) of Kaposi's sarcoma typically appear as painless purplish spots on the legs, feet or face. Lesions can also appear in the genital area, mouth or lymph nodes. CAUSE Human herpes virus 8 (HHV-8).
- 116. CONTINUED SYMPTOMS Slightly elevated purple, pink, brown, black, blue, or red blotches or bumps anywhere on the skin or in the mouth and/or throat, Lymphedema, which is swelling caused by a blockage of the lymphatic system, Unexplained cough or chest pain., Unexplained stomach or intestinal pain. DIAGNOSIS History collection, Physical examination, occult blood test, Chest x- ray, Brochoscopy, Colonoscopy.
- 117. PREVENTION Don't get sunburned. Avoid tanning, and never use UV tanning beds. Cover up with clothing, including a broad- brimmed hat and UV-blocking sunglasses. Use a broad-spectrum (UVA/UVB) sunscreen with an SPF of 15 or higher every day. Examine your skin for lesions. Consult your dermatologist.
- 118. CONTINUED TREATMENT Minor surgery (excision) Burning (electrodessication) or freezing (cryotherapy). Low-dose radiation, which is also helpful for lesions in the mouth. Injection of the chemotherapy drug vinblastine directly into lesions. Application of a vitamin A-like drug (retinoid).
- 119. CONCLUSION Skin is a tough, relatively impermeable, self-replacing organ that the body cannot easily live without. It provides protection and both sensory stimuli from the external environment. Skin cells which may have a short journey from the stratum basale to the stratum corneum, but the protective layer they leave behind lasts for a lifetime, endlessly protecting the body from injury and infectious organisms.
- 120. In today’s class we had discussed about Integumentary system Introduction of skin Definition Layers of skin Functions of skin Disorders of skin and their prevention
- 123. Q. Define skin. Ans. The body’s basic defense covering, which protects against heat and light, injury and infection.
- 124. Q. Enlist the name of the layers of skin. Ans. Epidermis Dermis Hypodermis (subcutaneous layer)
- 125. Q. Describe the functions of skin. Ans. Heat regulation Sensation Protection Absorption Excretion Secretion Vitamin D production
- 126. Q. Enlist the disorders of skin. ANS. HUMAN PAPILLOMA VIRUS Herpes viruses Impetigo Cellulitis Ringworm and tinea pedis Dermatitis (atopic and contact) Psoriasis Burns Pressure ulcers Malignant tumors
- 127. Q. Explain about the management of dermatitis. ANS. Don't get sunburned. Avoid tanning, and never use UV tanning beds. Cover up with clothing, including a broad- brimmed hat and UV-blocking sunglasses. Use a broad-spectrum (UVA/UVB) sunscreen with an SPF of 15 or higher every day. Examine your skin for lesions. Consult your dermatologist.
- 128. ASSIGNMENT Draw the structure of skin and explain about its function.
- 129. BIBLIOGRAPHY Brannon, H. (2007, April 9). Skin Anatomy . Retrieved July 14, 2012. Brouhard, R. (2007, May 7). Layers of the Skin: The Body's Flowerbed.Retrieved from : Candi, E., Schmidt, R., &Melino, G. (2005). The Conified Envelope: A Model of Cell Death in the Skin. Nature Reviews Molecular Cell Biology, 6(4), 328-340. doi:10.1038/nrm1619 . King, D. (2012, March 7). Introduction to Skin Histology. Retrieved.