This document discusses the pathophysiology and management of burn patients. It covers:
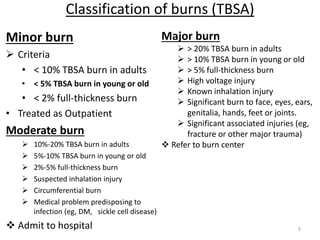
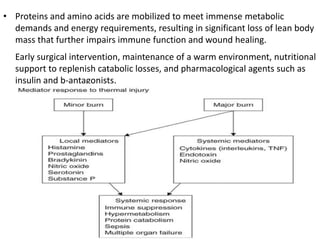
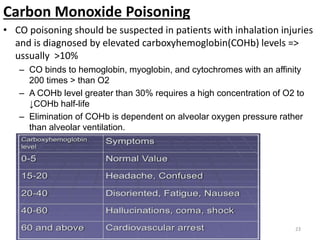
1) Major burns cause massive tissue destruction and inflammatory response, leading to burn shock from fluid shifts and systemic effects if >20% TBSA.
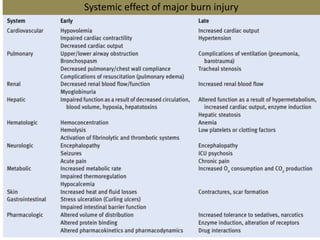
2) Burns trigger a hypermetabolic response for weeks, with increased cardiac work and protein catabolism impairing healing.
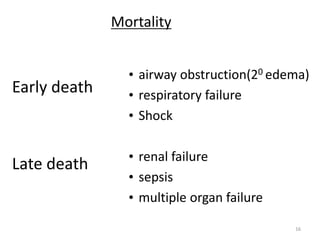
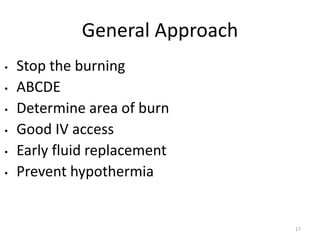
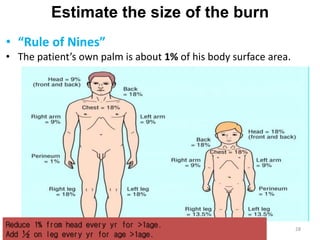
3) Resuscitation follows the Parkland formula to replace fluid losses. Fluid management aims to maintain urine output and prevent organ dysfunction.