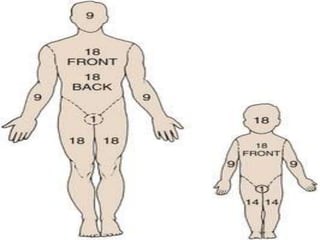
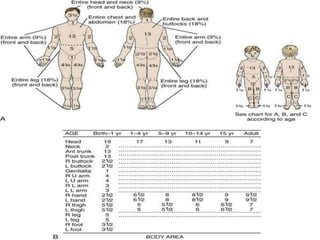
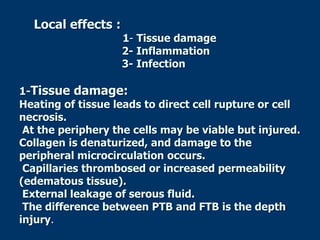
This document provides information on burns, including definitions, assessment, wound care, complications, and management. It defines burns as tissue damage caused by heat, chemicals, electricity, or radiation. Burn severity is assessed using factors like size, depth, and patient age/health. Wound care involves cleaning and dressing burns, with deeper burns requiring skin grafts. Complications can be local, such as infection, or systemic like fluid loss and organ failure. Management follows ABCDE protocol - Airway, Breathing, Circulation, Disability, Exposure. It also covers tetanus shots, antibiotics, wound care, physiotherapy and more.














![5.2 Burn[1]](https://cdn.slidesharecdn.com/ss_thumbnails/52-burn1-1202268563653474-3-thumbnail.jpg?width=640&height=640&fit=bounds)


















![nursing management of burn wounds.. [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/burns-classnotes-250310073133-5480c852-thumbnail.jpg?width=640&height=640&fit=bounds)















![Burns_UPDATED34566467567544433334[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/burnsupdated1-251001060239-3786d1e6-thumbnail.jpg?width=640&height=640&fit=bounds)




















