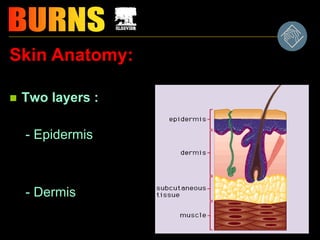
Skin Anatomy:
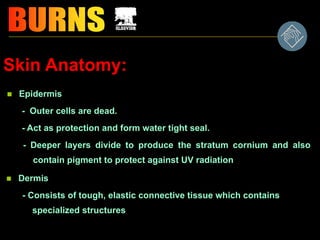
Epidermis
-Outer cells are dead.
- Act as protection and form water tight seal.
- Deeper layers divide to produce the stratum cornium and also
contain pigment to protect against UV radiation
Dermis
- Consists of tough, elastic connective tissue which contains
specialized structures
4.
Dermis -Specialized Structures:
- Nerve endings
- Blood vessels
- Sweat glands
- Oil glands - keep skin waterproof, usually
discharges around hair shafts
- Hair follicles - produce hair from hair root or papilla
• Each follicle has a small muscle (arrectus
pillorum) which can pull the hair upright and
cause goose flesh
5.
Skin physiology:
* Skinis the largest organ; it is complex and
multifunctional, containing many specialized cells
that are adapted to different functions .
6.
Skin physiology:
• Largestbody organ. Much more than a passive organ.
- Protects underlying tissues from injury.
- Temperature regulation.
- Acts as water tight seal, keeping body fluids in.
- Sensory organ.
- Vitamin - D formation
7.
• Burn woundsoccur when there is contact
between tissue and an energy source, such
as heat, chemicals, electrical current, or
radiation.
• The effects of the burn are influenced by the:
intensity of the energy
duration of exposure
type of tissue injured
8.
Types of BurnInjury
• Thermal burns: flame, flash, contact with hot objects.
• Scald burns: hot fluids.
• Chemical burns: necrotizing substances (acids, alkali).
• Electrical burns: intense heat from an electrical current
• Smoke & inhalation injury: inhaling hot air or noxious
chemicals
• Cold thermal injury: frostbite.
Chemical Burn
examples: cleaningagents...
Remember….
• Tissue destruction may continue for up to 72 hours.
• It is important to remove the person from the burning
agent or vice versa.
• The latter is accomplished by lavaging the affected area
with copious amounts of water.
Smoke and InhalationInjury
• Can damage the tissues of the respiratory
tract
• Although damage to the respiratory mucosa
can occur, it seldom happens because the
vocal cords and glottis closes as a
protective mechanisms.
Electrical Burns
• Injuryfrom electrical burns results from coagulation
necrosis that is caused by intense heat generated
from an electric current.
• The severity depends on:
Øamount of voltage
Øtissue resistance
Øcurrent pathways
Øsurface area in contact with the current
Ølength of time the current flow.
16.
Electrical injury cancause:
• Fractures of long bones and vertebra
• Cardiac arrest or arrhythmias--can be
delayed 24-48 hours after injury
• Severe metabolic acidosis--can develop in
minutes
• Myoglobinuria--acute renal tubular
necrosis.
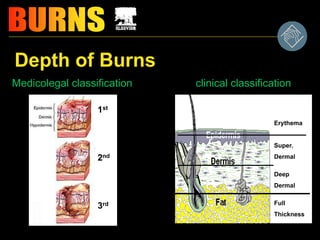
Classification of BurnInjury
Severity is determined by:
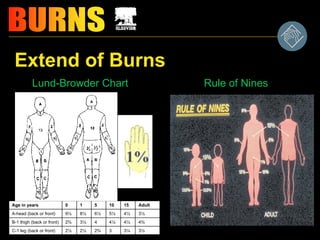
– depth of burn
– extend of burn calculated in percent of total body
surface (TBSA)
– location of burn
– patient risk factors
19.
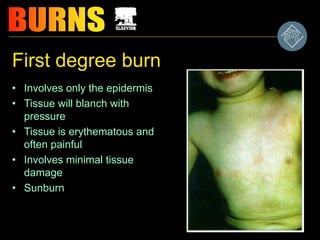
First degree burn
•Involves only the epidermis
• Tissue will blanch with
pressure
• Tissue is erythematous and
often painful
• Involves minimal tissue
damage
• Sunburn
20.
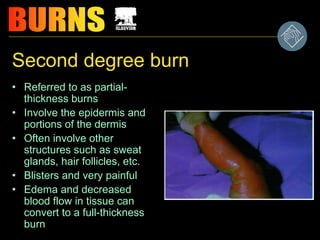
Second degree burn
•Referred to as partial-
thickness burns
• Involve the epidermis and
portions of the dermis
• Often involve other
structures such as sweat
glands, hair follicles, etc.
• Blisters and very painful
• Edema and decreased
blood flow in tissue can
convert to a full-thickness
burn
21.
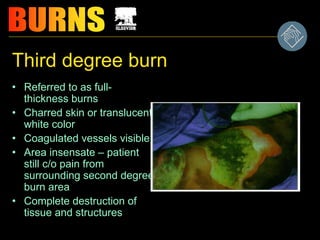
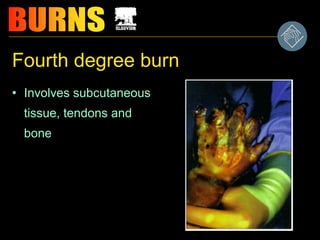
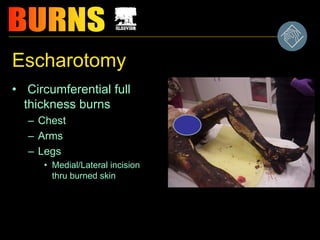
Third degree burn
•Referred to as full-
thickness burns
• Charred skin or translucent
white color
• Coagulated vessels visible
• Area insensate – patient
still c/o pain from
surrounding second degree
burn area
• Complete destruction of
tissue and structures
Phases of BurnManagement
_prehospital management
–emergent (resuscitative)
–acute
–rehabilitative
33.
Pre-hospital Care
• Removefrom area! Stop the burn!
• If thermal burn is large--FOCUS on
the ABC’s
A=airway-check for patency, soot
around nares, or signed nasal hair
B=breathing- check for adequacy of
ventilation
C=circulation-check for presence and
regularity of pulses
34.
Other precautions...
• Burntoo large--don’t immerse in water due to
extensive heat loss
• Never pack in ice
• P’t. should be wrapped in dry clean material
to decrease contamination of wound and
increase warmth.
35.
Emergent Phase (ResuscitativePhase)
• Lasts from onset to 5 or more days but
usually lasts 24-48 hours
• begins with fluid loss and edema formation
and continues until fluid motorization and
diuresis begins
• Greatest initial threat is hypovolemic
shock to a major burn patient!
36.
Management in theemergent phase is...
• Airway management-early nasotracheal or endotracheal
intubation before airway is actually compromised (usually 1-2
hours after burn)
• Ventilator.
• 6-12 hours later: Bronchoscopy to assess lower respiratory
tract
• chest physiotherapy and suction
37.
Complications during emergentphase
of burn injury are 3 major organ
systems...
–Cardiovascular
–Respiratory
–Renal systems
38.
Fluid Therapy
• 1or 2 large bore IV lines
• Fluid replacement based on:
– size/depth of burn
– age of pt.
– individualized considerations.
• options- RL, D5NS, dextan, albumin, etc.
• there are formula’s for replacement:
– Parkland formula
– Brooke formula
39.
Evans formula :-
1stday 1ml/kg/ %burn normal salin+ 1ml/kg/% burn coloid +
2000ccglucos
2nd day 0.5ml/kg/%burn saline+ 0.5ml/kg/% burn coloid +
2000cc
Brooks formula:-
1st day 2-3ml/kg * % burn RL + 2000CC GLUCOSE
2ND DAY 1ml/kg * % burn RL + 0.5 ML/KG *% BURN
COLLOID +2000cc glucose
Half the above formulae given during 1st 8 hours ,then other
half given during next 16 hours
It is to be noted that in all formulae , that maximum percent of
burn calculated is 50% to avoid serious over transfusion
40.
Assessing adequacy of
resuscitation
•Peripheral blood pressure:
may be difficult to obtain – often
misleading
• Urine Output: Best indicator
unless ARF occurs
• A-line: May be inaccurate due to
vasospasm
• CVP: Better indicator of fluid
status
• Heart rate: Valuable in early
post burn period – should be
around 120/min.
• > HR indicates need for >
fluids or pain control
• Invasive cardiac
monitoring: Indicated in a
minority of patients (elderly or
pre-existing cardiac disease)
Wound Care continued...
•Staff should wear disposable hats, gowns,
gloves, masks when wounds are exposed
• appropriate use of sterile vs. nonsterile
techniques
• keep room warm
• careful handwashing
• any bathing areas disinfected before and
after bathing
44.
Other care measuresinclude
• Face
– eye
– ear
• Hands & arms
• Perineum
• Physiotherapy
45.
Drug Therapy
• Analgesicsand Sedatives
• Tetanus immunization
• Antimicrobial agents: Silver sulfadiazine
Nutritional Therapy
• Burn patients need more calories & failure
to provide will lead to delayed wound
healing and malnutrition.
46.
IN YOUR MINDS:
• Burn wound either heals by primary
intention or by grafting.
• Scars may form & contractures.
• Mature healing is reached in 6
months to 2 years
• Avoid direct sunlight for 1 year on
burn
• new skin sensitive to trauma
47.
Care of BU R N S
B - breathing
U - urine output
R - rule of nines
resuscitation of fluid
N - nutrition
S - shock
silvadene
48.
Associated Trauma
• SpinalInjuries
• Airway Trauma
• Chest Trauma/Baro Trauma
• Abd. Trauma
• CHI
• Open wounds/Fractures/Shrapnel
• Shock
• If you find a Hypotensive acute burn Patient,
there is something else you are missing!
49.
Aims from semner
*Understandthe basic anatomy and
*function of the skin
*Identify the types of common burn
trauma
*Accurately assess the burn severity,
and common progression of patient
condition
*Identify co morbid factors