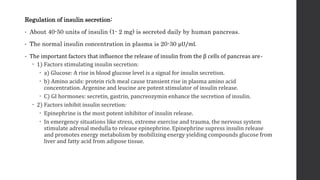
The document provides an overview of diabetes mellitus, emphasizing the role of insulin in glucose metabolism and its types, including Type I and Type II diabetes. Insulin, a peptide hormone produced by pancreatic β-cells, is vital for regulating nutrient storage and utilization, and its synthesis involves the precursor proteins preproinsulin and proinsulin. It also discusses the factors influencing insulin secretion and its mechanisms of action, along with details on insulin preparations used for therapeutic purposes.

































![INSULIN AND OTHER ANTIDIABETEC DRUGS [Autosaved] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/insulinandotherantidiabetecdrugsautosavedautosaved-220731124033-32b4f1bb-thumbnail.jpg?width=640&height=640&fit=bounds)






![anti diabetics [Autosaved] final.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/antidiabeticsautosavedfinal-231210163451-81c335f7-thumbnail.jpg?width=640&height=640&fit=bounds)






























