This document discusses amniotic fluid, including its:
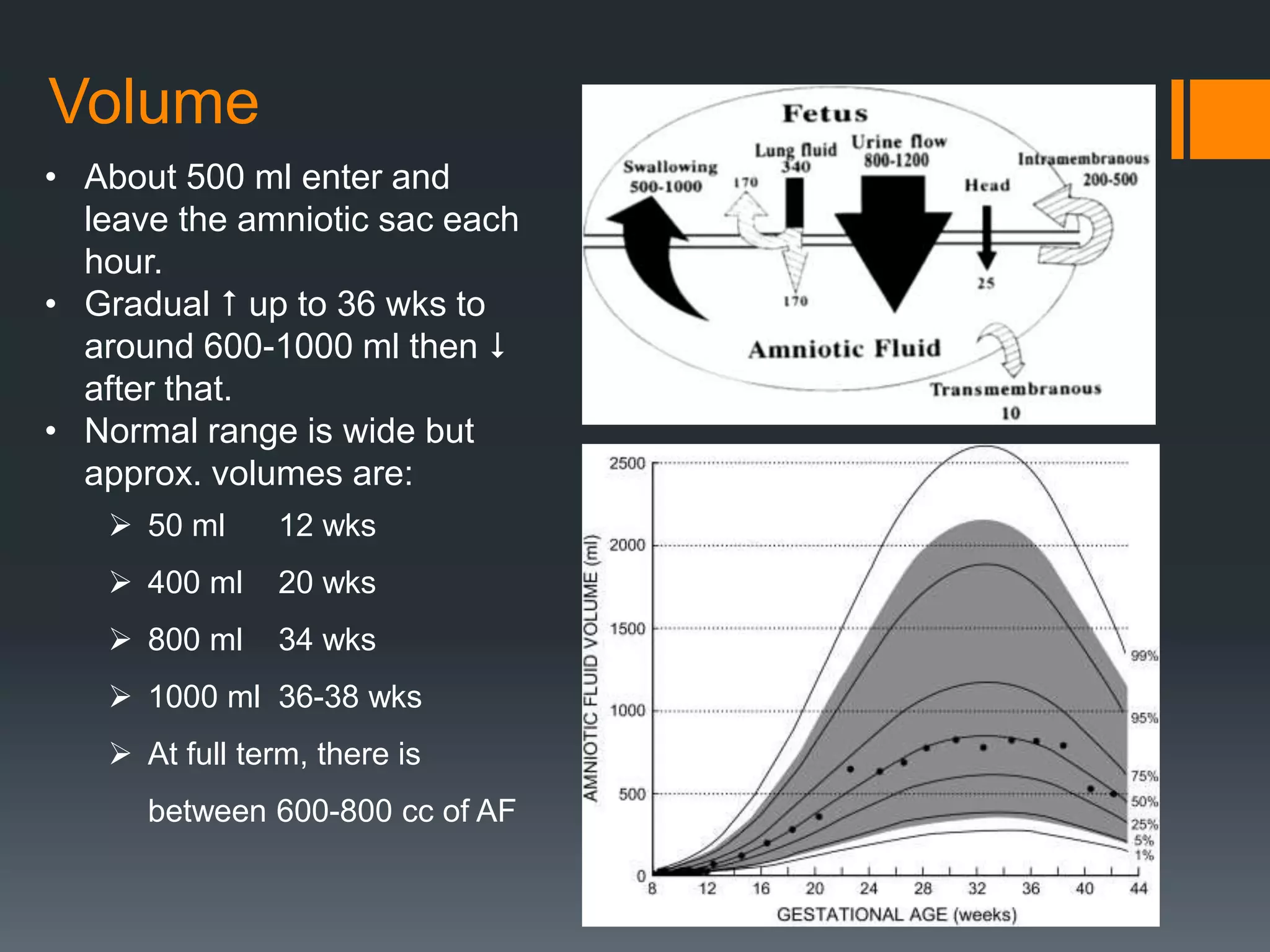
- Volume, which increases to around 1000 ml by 36-38 weeks gestation before decreasing.
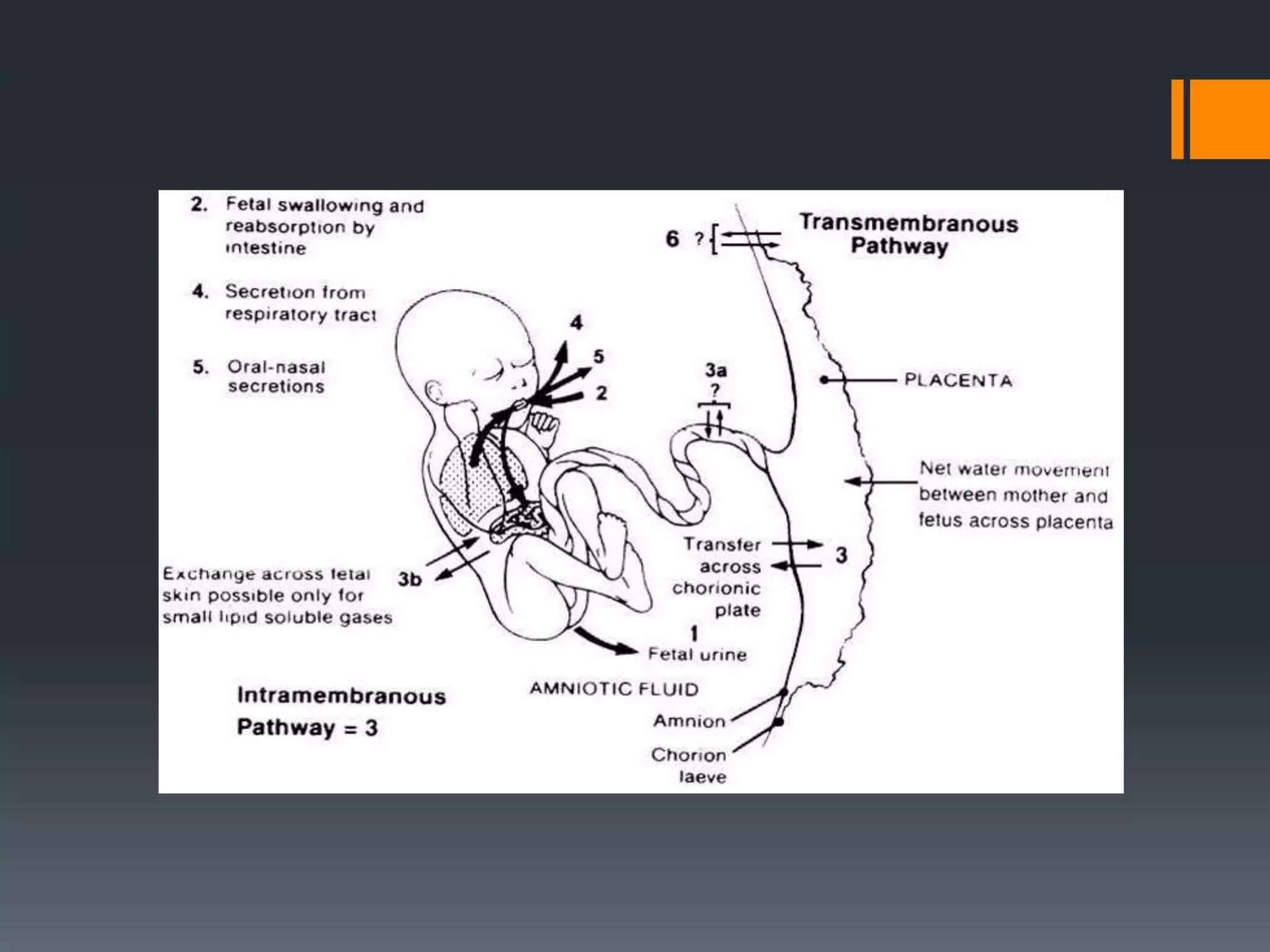
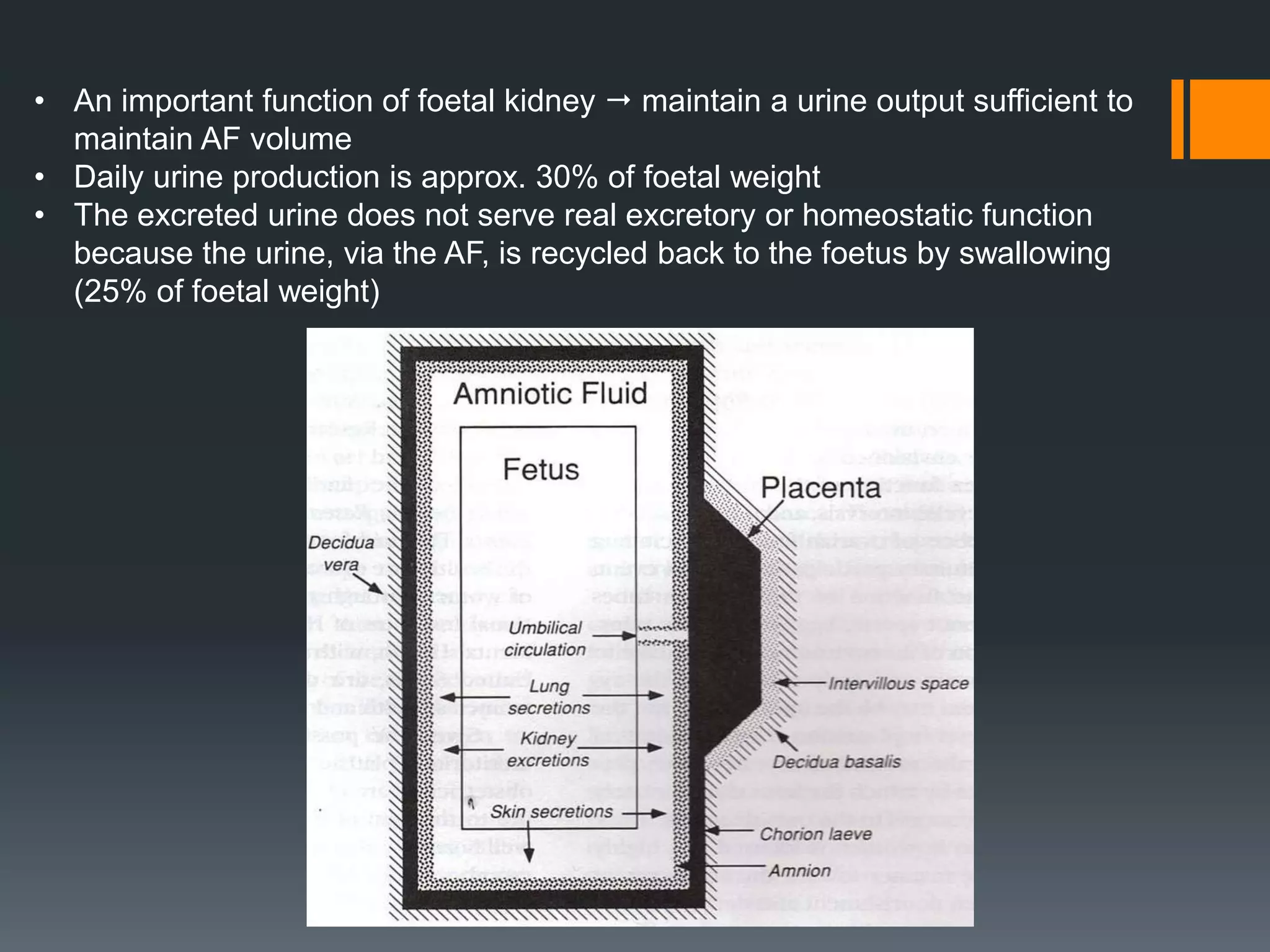
- Circulation and constituents, which originate from both the mother and fetus through processes like transudation, secretion, swallowing, and fetal urination.
- Composition, which changes with gestation and includes water, electrolytes, urea, and other substances from the fetus.
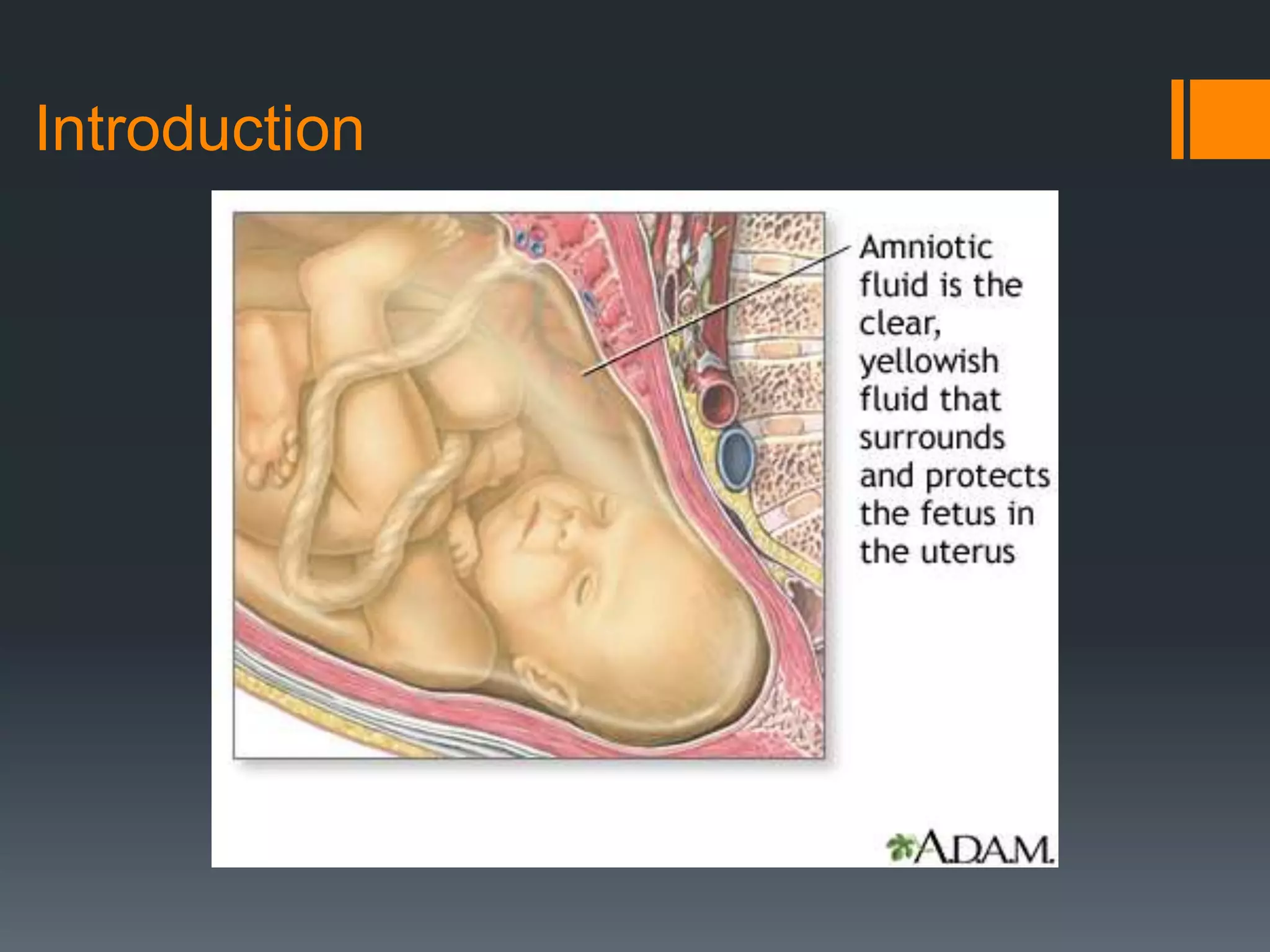
- Functions in allowing fetal movement, aiding lung and bone development, maintaining temperature, and protecting the fetus.
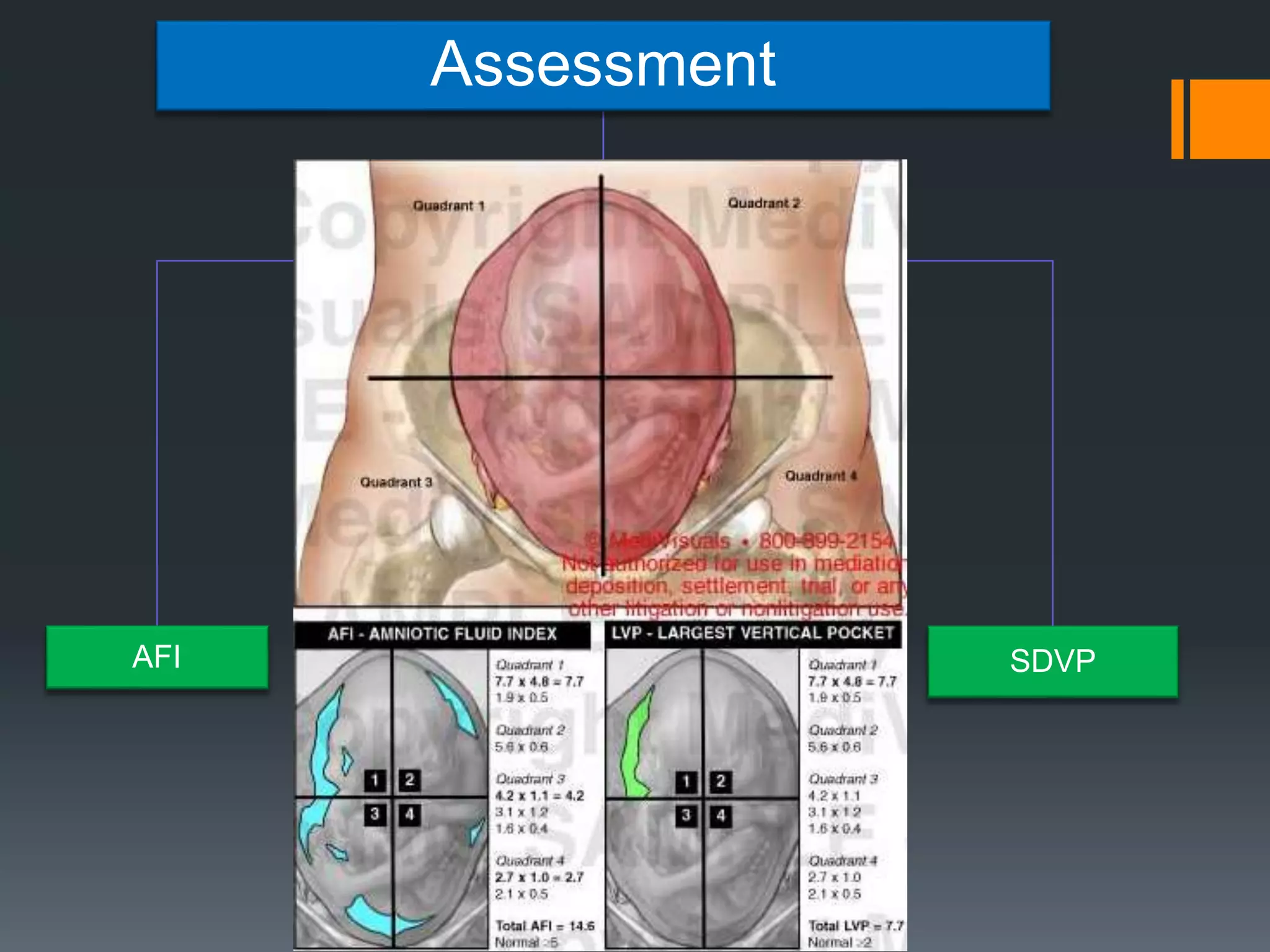
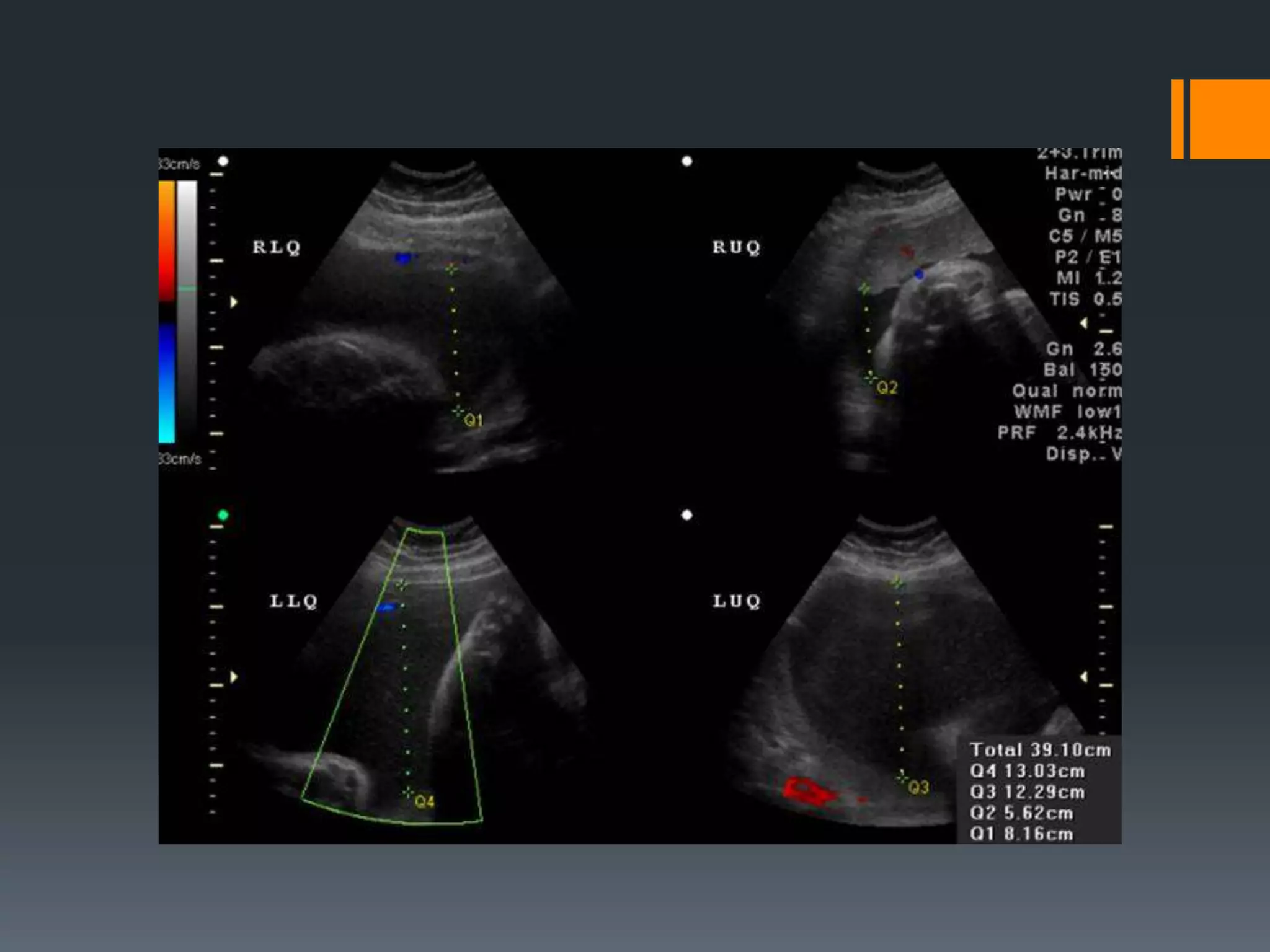
- Assessment methods like measuring the single deepest vertical pocket (SDVP) and amniotic fluid index (AFI).