Downloaded 65 times











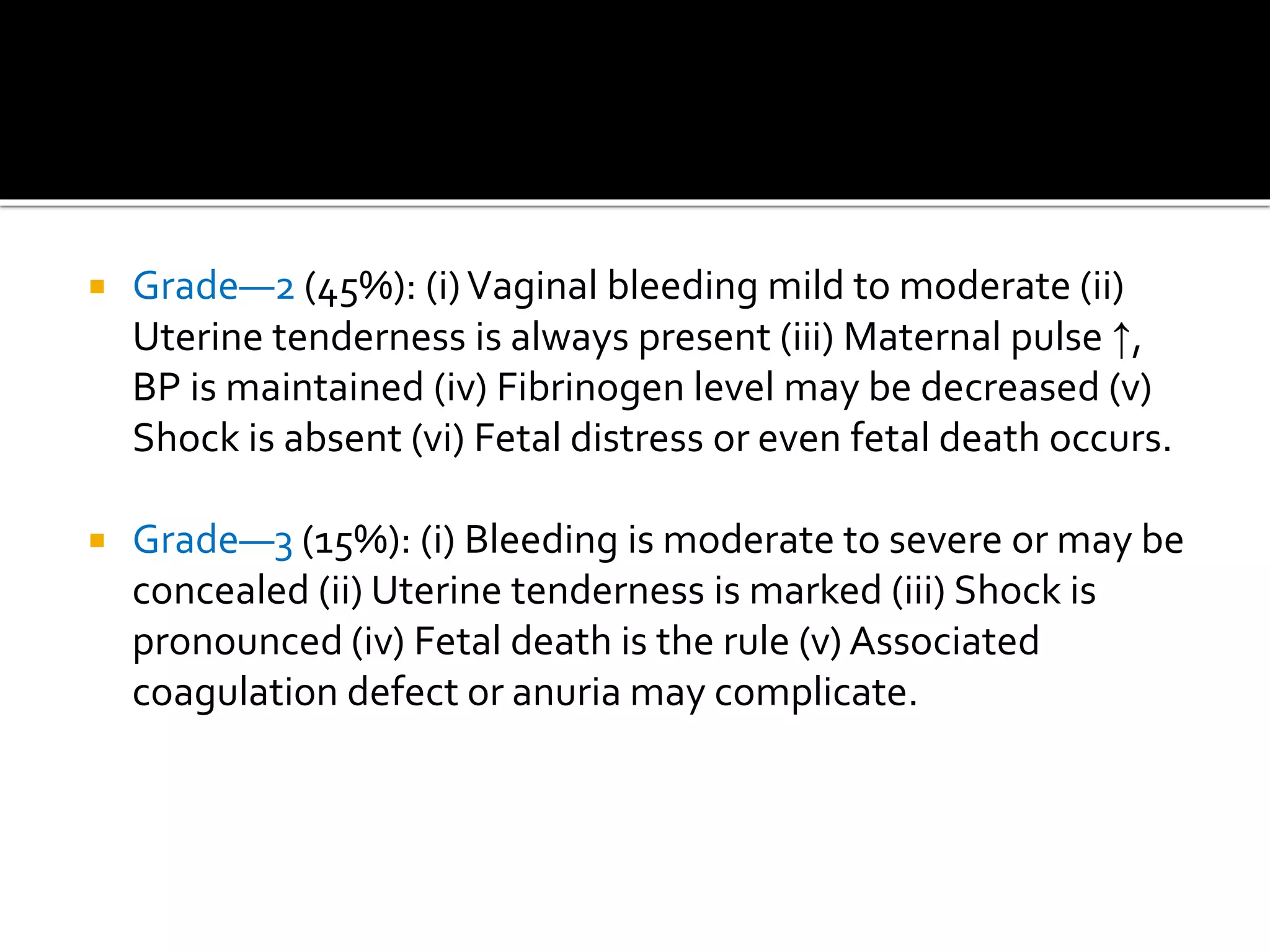
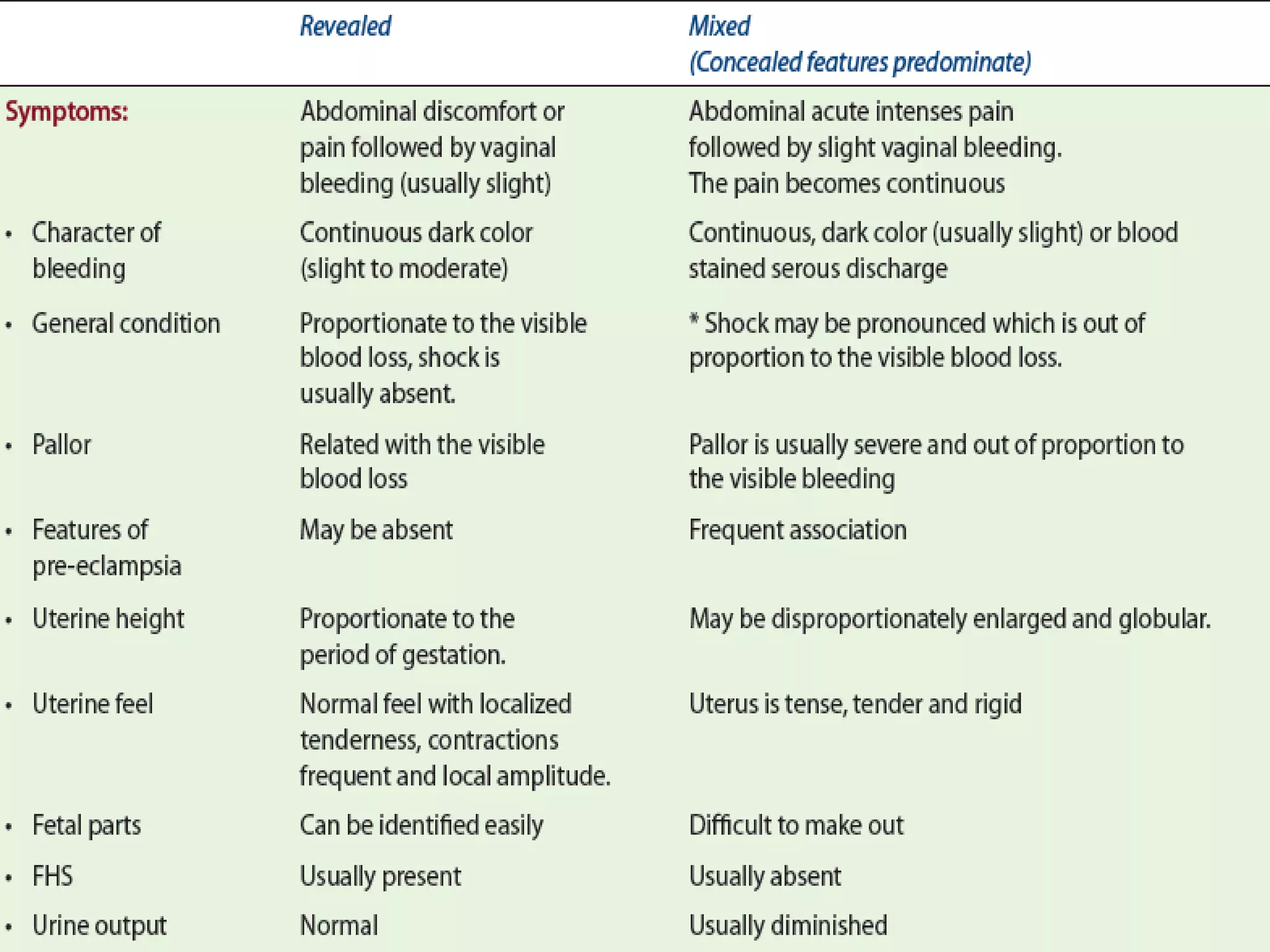














Placental abruption occurs when the placenta detaches from the uterus prior to delivery of the baby. It can lead to significant maternal and neonatal morbidity and mortality. Risk factors include hypertension, smoking, and prior abruption. Symptoms may include vaginal bleeding, abdominal pain, and changes in fetal heart rate. Ultrasound can show a retroplacental hematoma. Management involves monitoring, administering medications to help the baby's lungs/brain if preterm, and delivery depending on gestational age and stability of the mother and baby. Women with a history of abruption have a higher risk of recurrence.





































![obstetric 2 lecture note for health].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/l-1bleedinginlatepregnancy1-240604192427-51f7250b-thumbnail.jpg?width=640&height=640&fit=bounds)








![obstetric 1 antinatal care for midwifery].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/l-1bleedinginlatepregnancy1-240604190707-264c2efa-thumbnail.jpg?width=640&height=640&fit=bounds)








































