


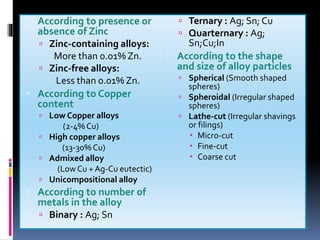
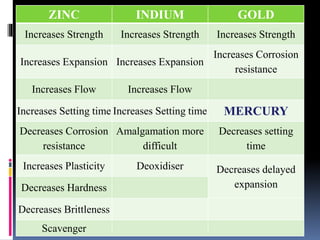
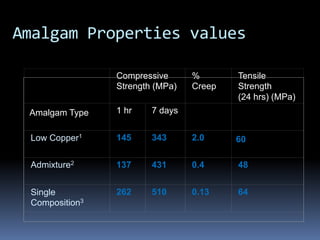

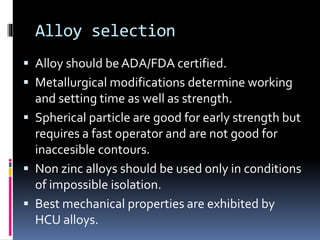
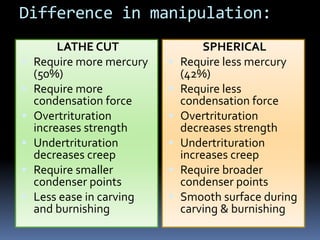
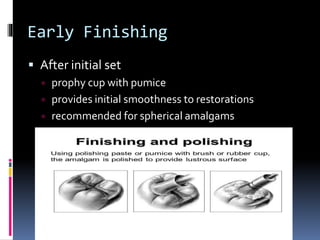






This document provides an overview of dental amalgam, including its: - Classification based on composition and particle shape - Generations and typical compositions - Properties including strength, creep, corrosion resistance - Toxicity and mercury levels - Manipulation techniques for mixing, condensing, and finishing amalgam restorations - Status and concerns about mercury levels from dental offices



































































