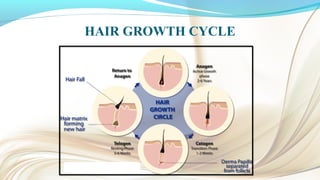
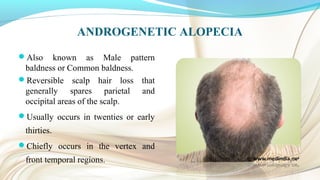
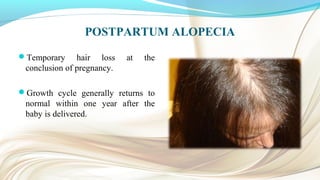
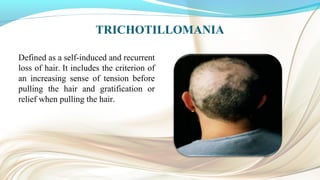
Hairs project from the body's surface and come in a variety of lengths, widths, and growth rates. They serve protective, sensory, and social functions. Hair growth occurs in cycles of anagen, catagen, telogen, and exogen phases. Common types of hair loss include alopecia areata (patchy bald spots), androgenetic alopecia (male or female pattern baldness), and postpartum alopecia. Hair loss can be caused by physical or emotional stress, diet, hormones, medical conditions, or hair manipulation. Treatments include corticosteroids, minoxidil, finasteride, behavior modification, and hair implants.