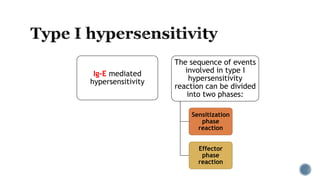
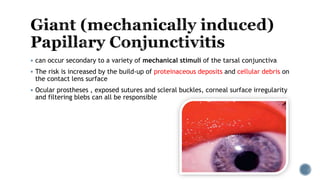
This document discusses ocular allergies and allergic conjunctivitis. It begins by defining allergy and hypersensitivity. It then discusses the different types of allergic conjunctivitis including seasonal, perennial, vernal keratoconjunctivitis (VKC), atopic keratoconjunctivitis (AKC), and giant papillary conjunctivitis (GPC). For each type it describes the pathogenesis, clinical features, and treatment approaches. It also covers the pathophysiology of type I hypersensitivity reactions and summarizes the goals of understanding ocular allergies, identifying causes and symptoms of allergic conjunctivitis, recognizing different allergic eye diseases, discussing treatment drugs, and