1. Viral corneal ulcers have increased due to antibiotics reducing bacterial flora. Herpes simplex virus is a common cause, initially infecting epithelium and potentially becoming neurotropic. Primary infection involves non-immune individuals while recurrent infections reactivate dormant virus.
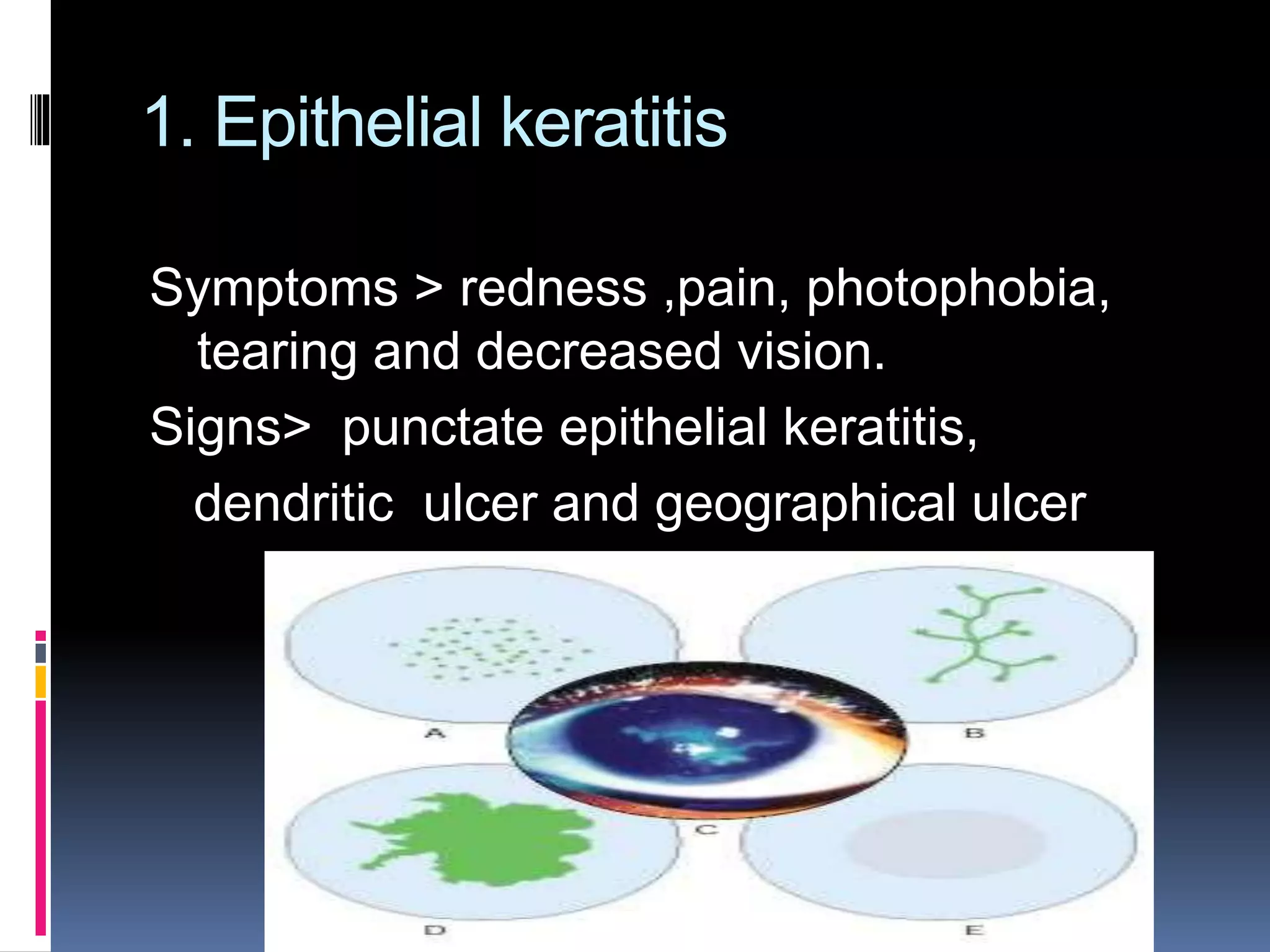
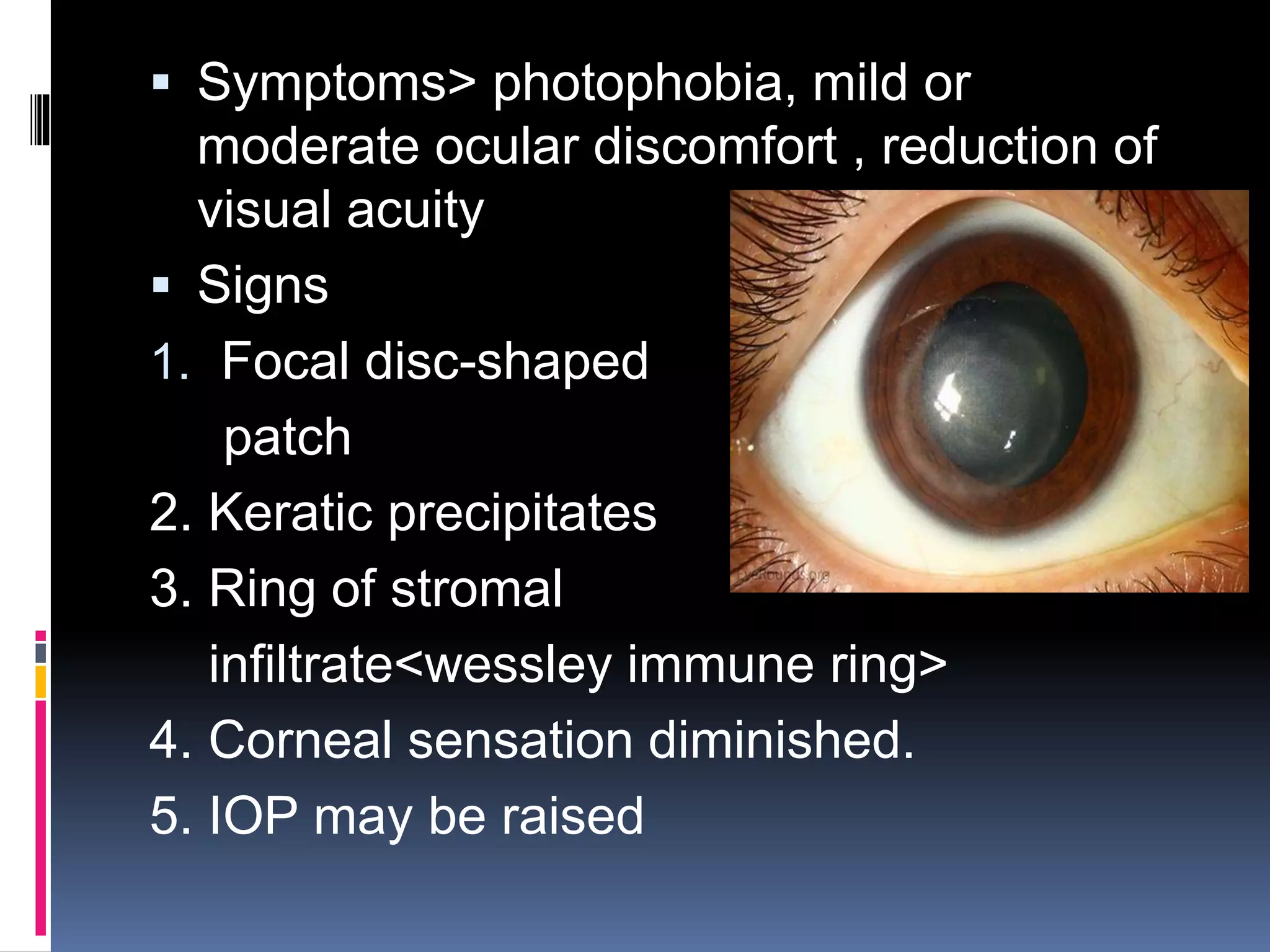
2. Herpes simplex keratitis manifestations include punctate epithelial keratitis, dendritic ulcers, and stromal keratitis treated with antivirals like acyclovir along with supportive measures. Herpes zoster ophthalmicus affects the trigeminal nerve causing vesicular skin lesions and ocular complications in 50% of cases like keratitis, treated with antivirals and steroids.