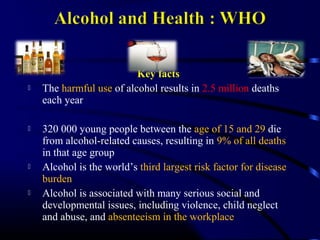

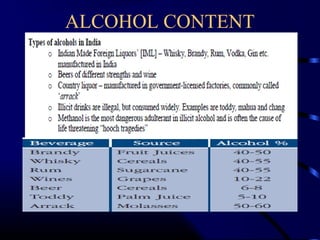

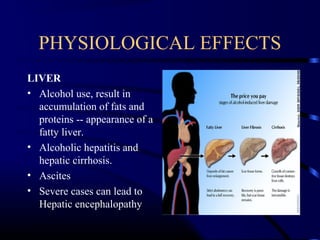
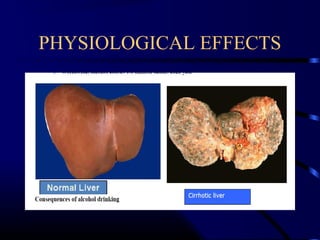
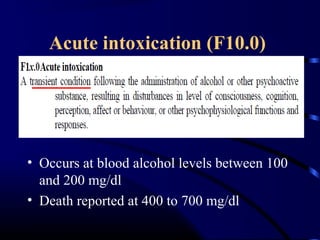



The document discusses alcohol use disorders and management. Some key points: - Alcohol use results in 2.5 million deaths annually worldwide, especially among youth. - India's alcohol consumption is increasing, especially in certain states, and the average age of initiation is declining. - Alcohol dependence is diagnosed based on criteria including withdrawal symptoms and tolerance. - Withdrawal can cause tremors, seizures, delirium tremens and is managed with benzodiazepines. - Long-term effects include liver disease, brain damage and increased risk of certain cancers.