- Alcohol use disorders, including dependence and abuse, affect about 13% of the world population. Alcohol causes around 3.8% of deaths worldwide and 4.5% of disability-adjusted life years.
- There is a causal relationship between alcohol consumption and over 60 types of diseases and injuries. Some cancers and injuries caused by alcohol account for 20-30% of cases worldwide.
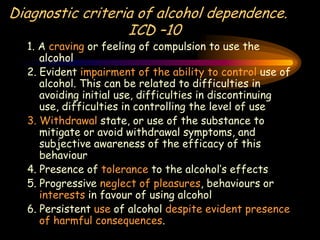
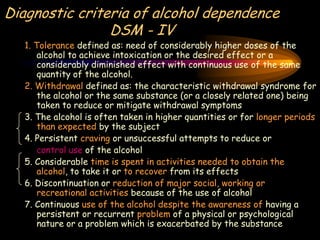
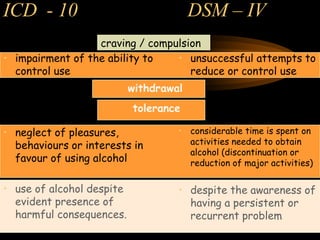
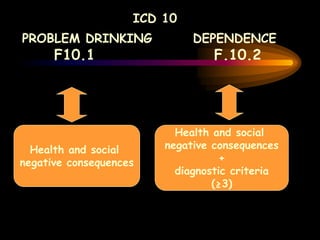
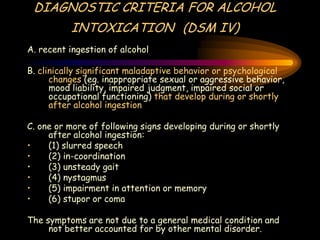
- Diagnostic criteria for alcohol dependence include tolerance, withdrawal symptoms, inability to control use, and continuing use despite harms. Dependence is associated with changes in brain regions involved in reward and inhibition.