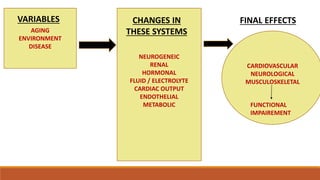
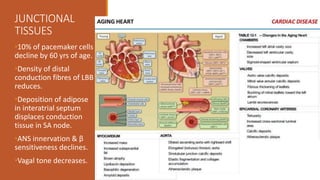
1. The cardiovascular system undergoes several age-related changes that affect the body's physiology in elderly people. This includes increased thickening and stiffness of blood vessels, endothelial damage reducing nitric oxide production, and changes to junctional tissues reducing conduction abilities.
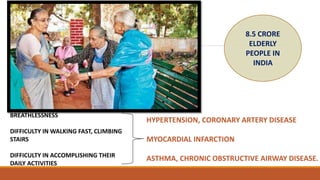
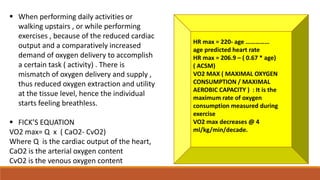
2. These structural changes, along with other risk factors, lead to physiological changes like elevated blood pressure, reduced cardiac output, decreased aerobic capacity and oxygen exchange at tissues. As a result, elderly individuals more easily experience breathlessness during physical exertion.
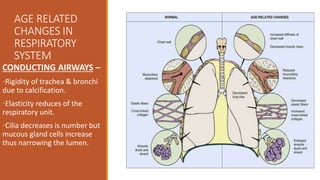
3. The respiratory system also exhibits age-related changes that increase the work of breathing and decrease lung function parameters, further contributing to breathlessness in the elderly.