Advanced haemodynamic monitoring involves closely monitoring parameters of the circulatory system such as preload, contractility, and afterload. This summary provides an overview of some key aspects of advanced haemodynamic monitoring discussed in the document:
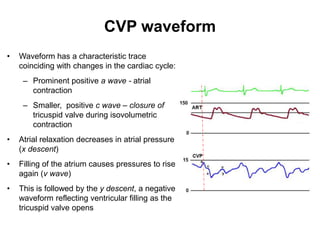
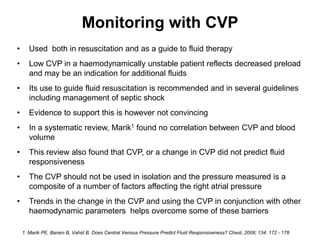
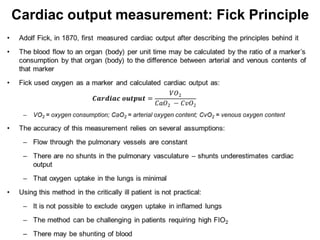
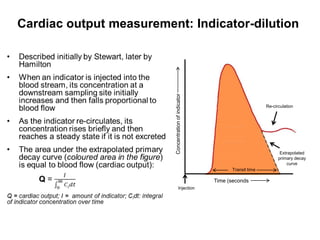
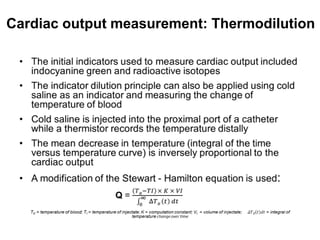
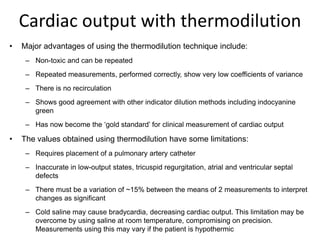
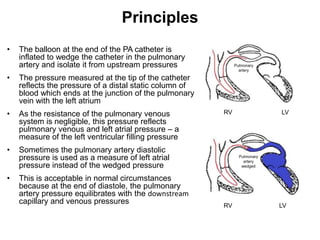
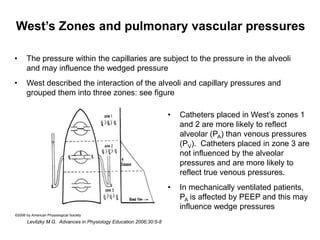
Central venous pressure (CVP) monitoring is commonly used but CVP is an indirect measure influenced by many factors and does not always accurately reflect cardiac preload. Cardiac output can be measured using techniques such as thermodilution which involves injecting cold saline through a pulmonary artery catheter. Pulmonary artery catheters allow measurement of pulmonary pressures and cardiac output but require an invasive procedure and have some limitations. Advanced monitoring provides more detailed information than basic monitoring but also has greater risks and limitations









![Anaesthesia for cardiopulmonary bypass surgery [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/anaesthesiaforcardiopulmonarybypasssurgeryautosaved-150531185352-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)









































