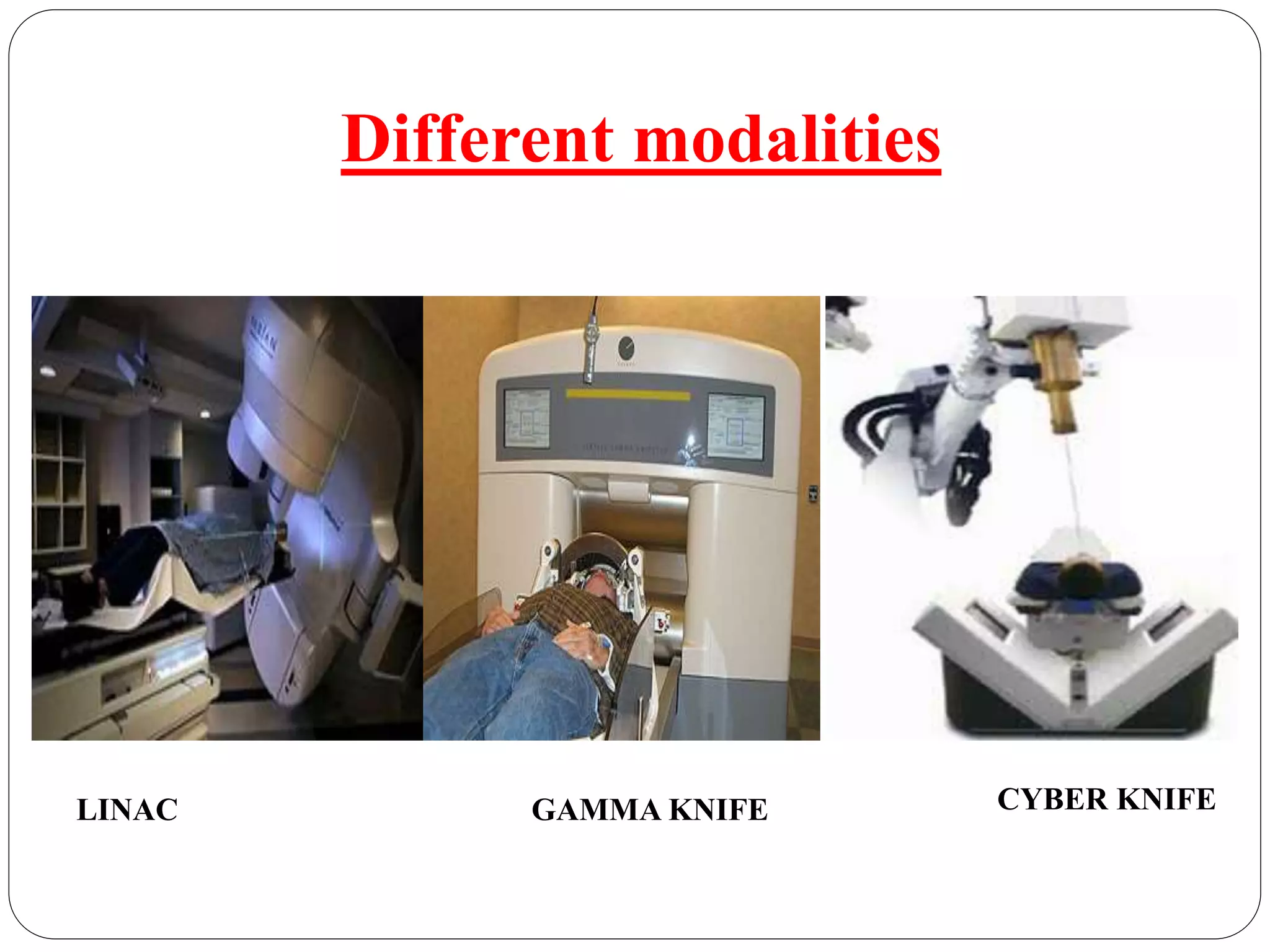
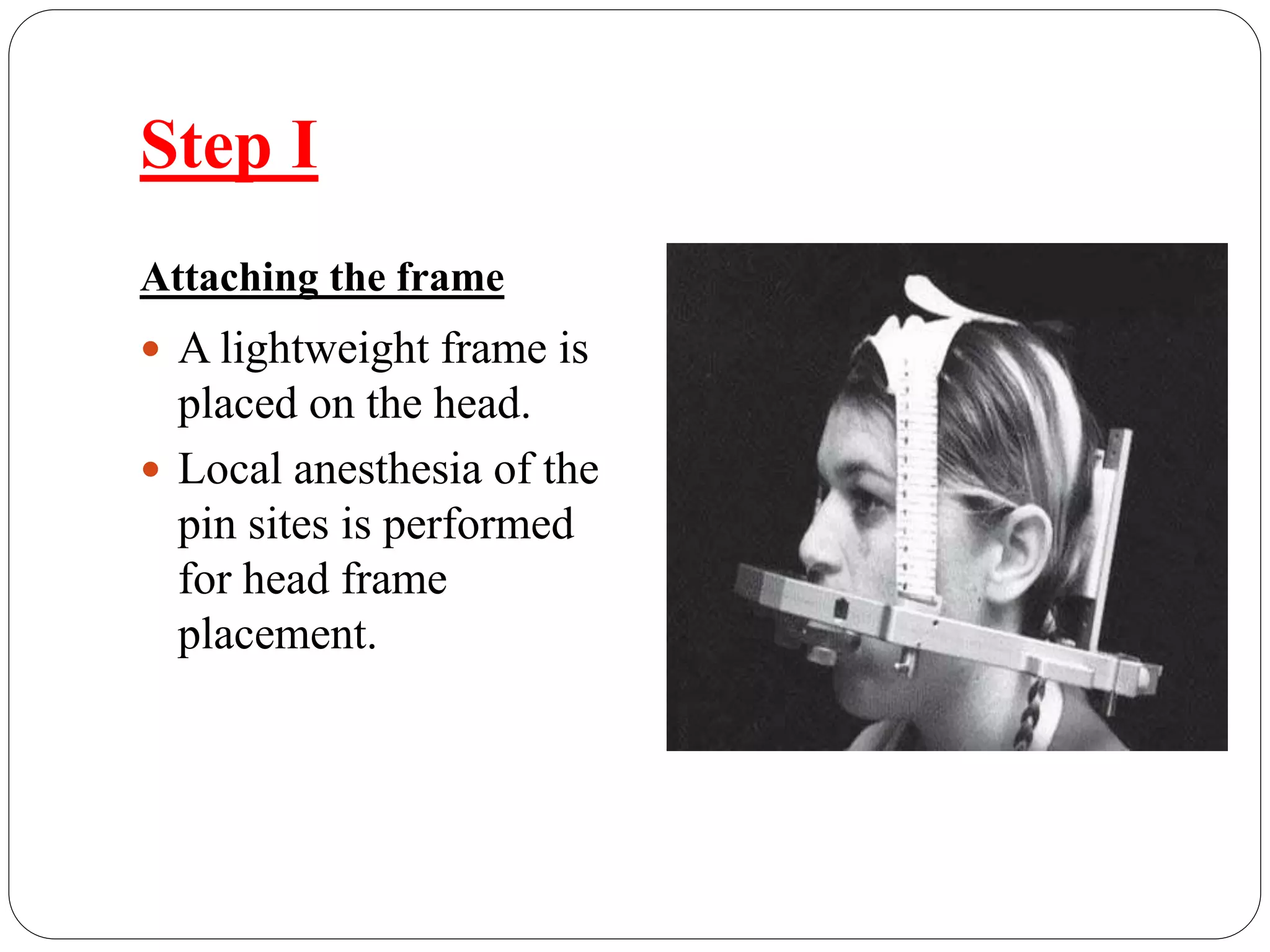
This document discusses intracranial stereotactic radiosurgery (SRS), which precisely delivers a high dose of radiation to lesions in the brain or skull base in a single session as an alternative to surgery. It was invented in Sweden using the Gamma Knife device. SRS involves attaching a frame to the head for imaging and planning treatment using LINAC, Gamma Knife, or Cyber Knife machines. Common indications are brain metastases, meningiomas, and acoustic neuromas, while contraindications include large or eloquent area tumors. The treatment process involves frame placement, imaging, planning, and a single high-dose radiation session while awake. SRS offers advantages over surgery like reduced risks and